

Intratumoral heterogeneity as a therapy resistance mechanism: role of melanoma subpopulations
- PMID: 22959031
- PMCID: PMC3677516
- DOI: 10.1016/B978-0-12-397927-8.00011-7
Intratumoral heterogeneity as a therapy resistance mechanism: role of melanoma subpopulations
Abstract
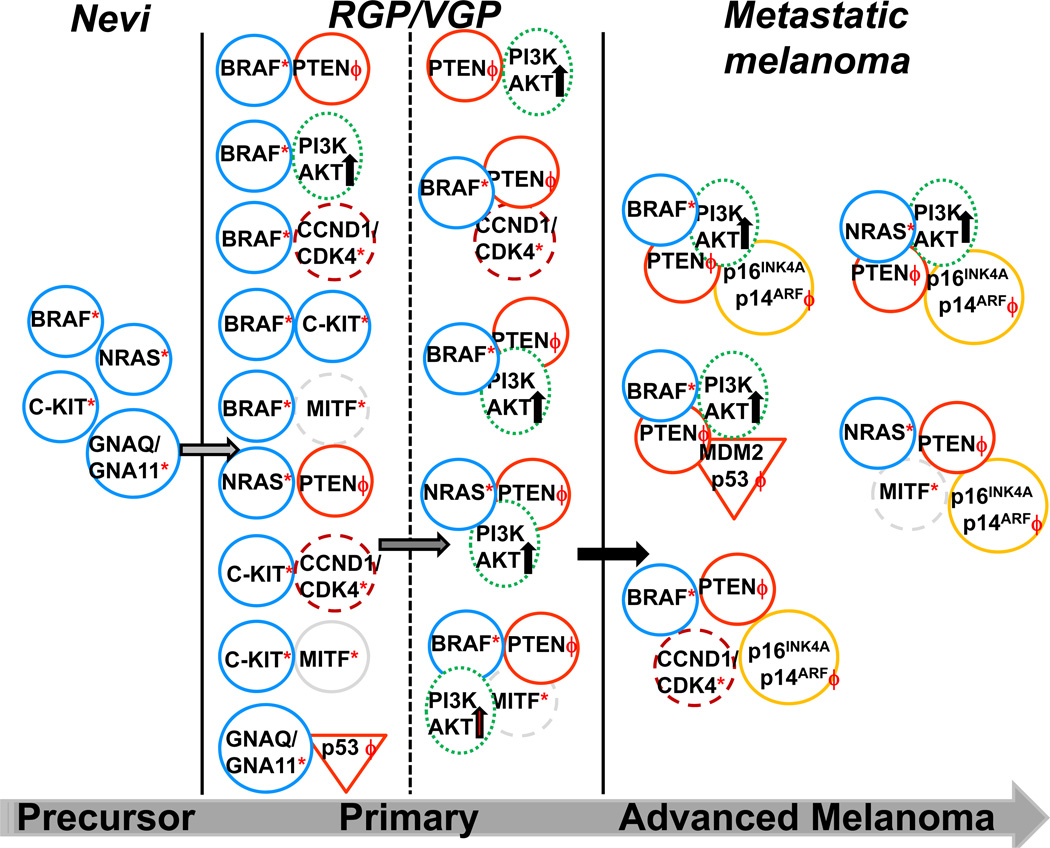
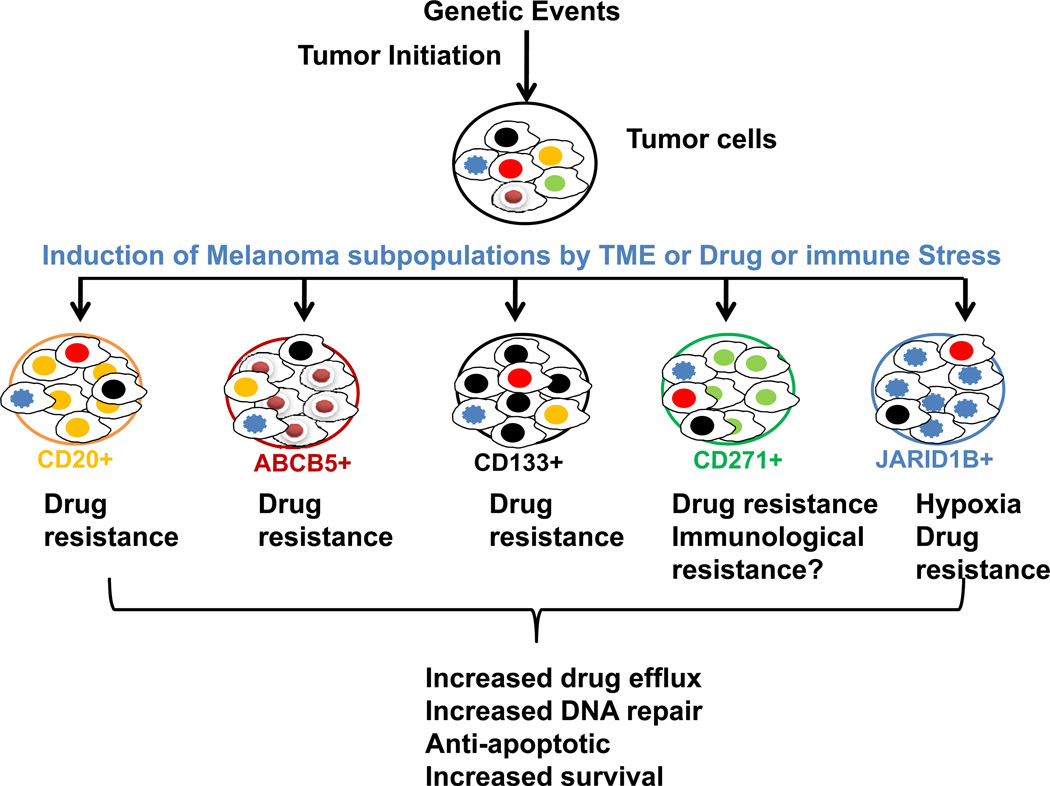
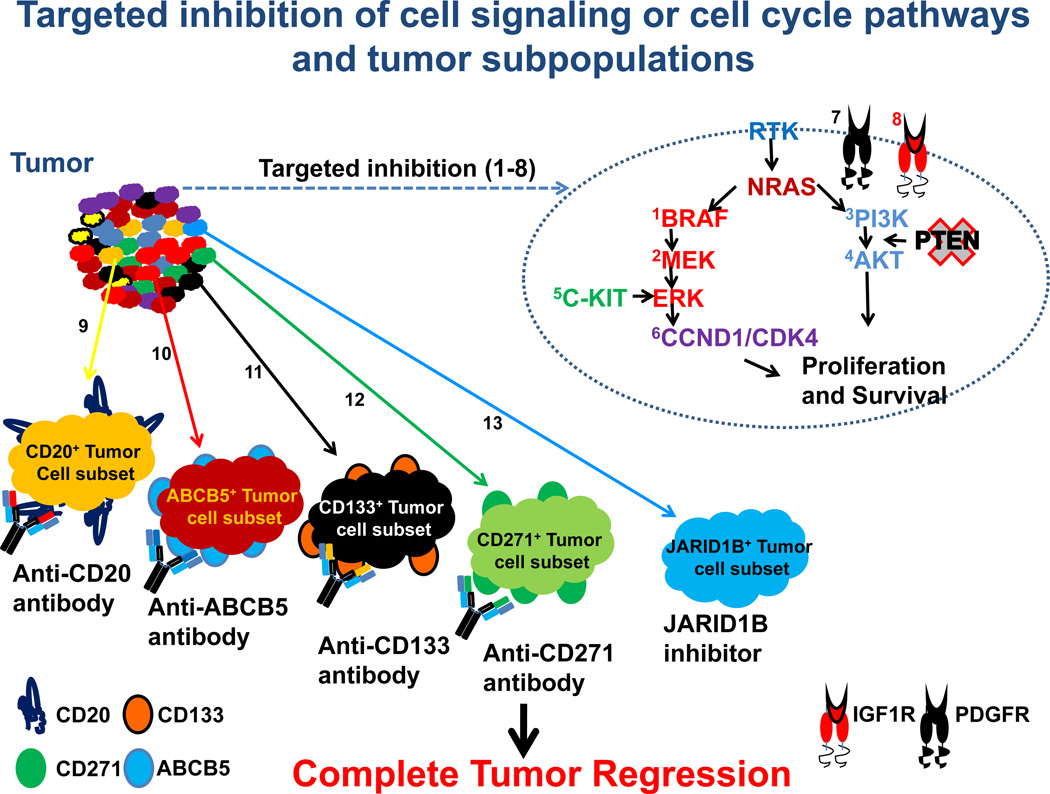
Malignant melanoma is an aggressive form of skin cancer whose incidence continues to increase worldwide. Increased exposure to sun, ultraviolet radiation, and the use of tanning beds can increase the risk of melanoma. Early detection of melanomas is the key to successful treatment mainly through surgical excision of the primary tumor lesion. But in advanced stage melanomas, once the disease has spread beyond the primary site to distant organs, the tumors are difficult to treat and quickly develop resistance to most available forms of therapy. The advent of molecular and cellular techniques has led to a better characterization of tumor cells revealing the presence of heterogeneous melanoma subpopulations. The discovery of gene mutations and alterations of cell-signaling pathways in melanomas has led to the development of new targeted drugs that show dramatic response rates in patients. Single-agent therapies generally target one subpopulation of tumor cells while leaving others unharmed. The surviving subpopulations will have the ability to repopulate the original tumors that can continue to progress. Thus, a rational approach to target multiple subpopulations of tumor cells with a combination of drugs instead of single-agent therapy will be necessary for long-lasting inhibition of melanoma lesions. In this context, the recent development of immune checkpoint reagents provides an additional armor that can be used in combination with targeted drugs to expand the presence of melanoma reactive T cells in circulation to prevent tumor recurrence.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
The other authors disclosed no potential conflicts of interest.
Figures
References
-
- Albini A, Mirisola V, Pfeffer U. Metastasis signatures: genes regulating tumormicroenvironment interactions predict metastatic behavior. Cancer Metastasis Rev. 2008;27(1):75–83. - PubMed
-
- Augustine CK, Yoo JS, Potti A, Yoshimoto Y, Zipfel PA, Friedman HS, et al. Genomic and molecular profiling predicts response to temozolomide in melanoma. Clin Cancer Res. 2009;15(2):502–510. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
