

How much muscle strength is required to walk in a crouch gait?
- PMID: 22959837
- PMCID: PMC3524281
- DOI: 10.1016/j.jbiomech.2012.07.028
How much muscle strength is required to walk in a crouch gait?
Abstract
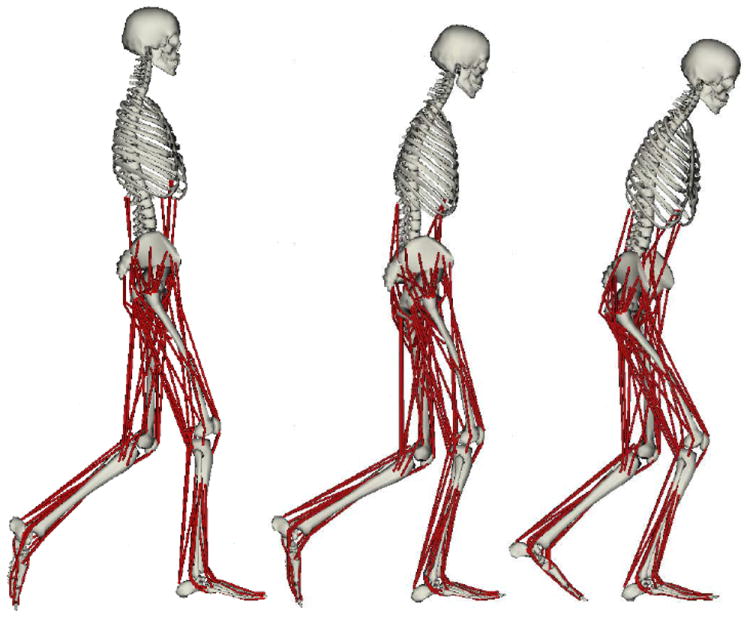
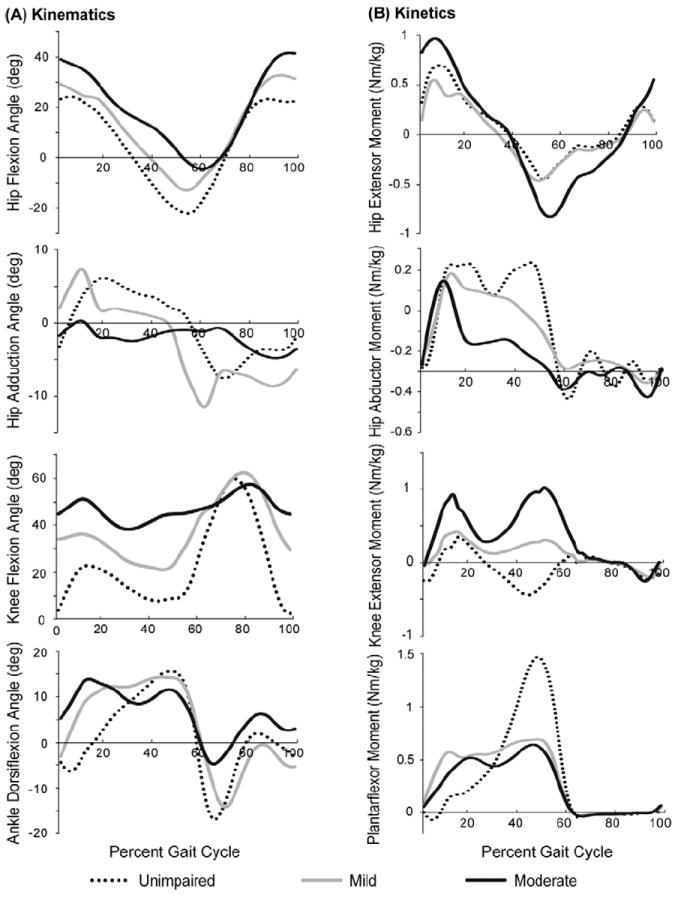
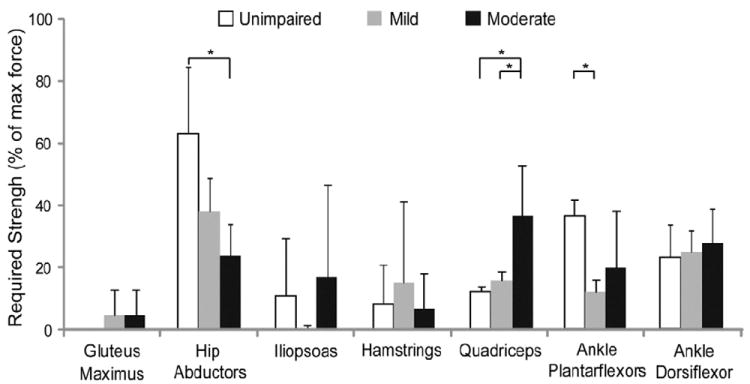
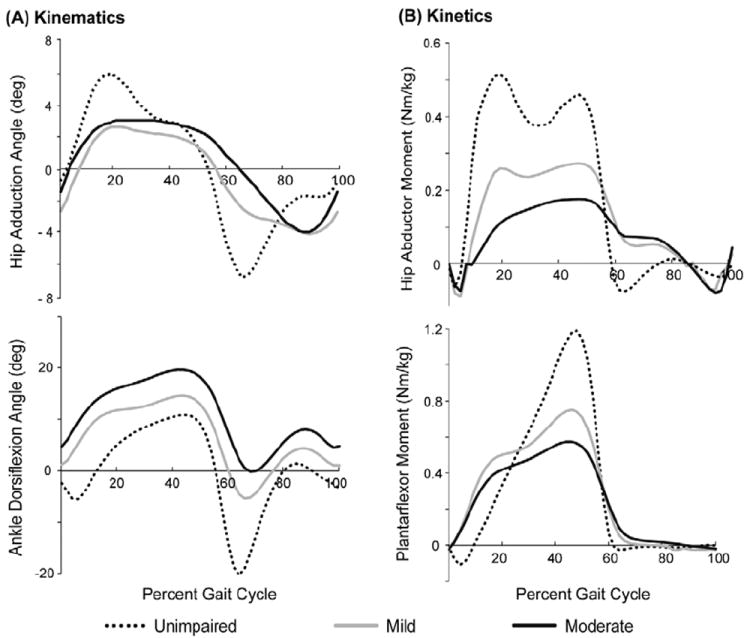
Muscle weakness is commonly cited as a cause of crouch gait in individuals with cerebral palsy; however, outcomes after strength training are variable and mechanisms by which muscle weakness may contribute to crouch gait are unclear. Understanding how much muscle strength is required to walk in a crouch gait compared to an unimpaired gait may provide insight into how muscle weakness contributes to crouch gait and assist in the design of strength training programs. The goal of this study was to examine how much muscle groups could be weakened before crouch gait becomes impossible. To investigate this question, we first created muscle-driven simulations of gait for three typically developing children and six children with cerebral palsy who walked with varying degrees of crouch severity. We then simulated muscle weakness by systematically reducing the maximum isometric force of each muscle group until the simulation could no longer reproduce each subject's gait. This analysis indicated that moderate crouch gait required significantly more knee extensor strength than unimpaired gait. In contrast, moderate crouch gait required significantly less hip abductor strength than unimpaired gait, and mild crouch gait required significantly less ankle plantarflexor strength than unimpaired gait. The reduced strength required from the hip abductors and ankle plantarflexors during crouch gait suggests that weakness of these muscle groups may contribute to crouch gait and that these muscle groups are potential targets for strength training.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Conflict of interest statement
None of the authors had financial or personal conflict of interest with regard to this study.
Figures
Similar articles
-
Muscle contributions to vertical and fore-aft accelerations are altered in subjects with crouch gait.Gait Posture. 2013 May;38(1):86-91. doi: 10.1016/j.gaitpost.2012.10.019. Epub 2012 Nov 27. Gait Posture. 2013. PMID: 23200083 Free PMC article.
-
Individual muscle force-energy rate is altered during crouch gait: A neuro-musculoskeletal evaluation.J Biomech. 2022 Jun;139:111141. doi: 10.1016/j.jbiomech.2022.111141. Epub 2022 May 17. J Biomech. 2022. PMID: 35609492
-
Muscle contributions to support and progression during single-limb stance in crouch gait.J Biomech. 2010 Aug 10;43(11):2099-105. doi: 10.1016/j.jbiomech.2010.04.003. Epub 2010 May 20. J Biomech. 2010. PMID: 20493489 Free PMC article.
-
Characteristics associated with improved knee extension after strength training for individuals with cerebral palsy and crouch gait.J Pediatr Rehabil Med. 2012;5(2):99-106. doi: 10.3233/PRM-2012-0201. J Pediatr Rehabil Med. 2012. PMID: 22699100 Free PMC article. Review.
-
Crouch gait or flexed-knee gait in cerebral palsy: Is there a difference? A systematic review.Gait Posture. 2020 Oct;82:153-160. doi: 10.1016/j.gaitpost.2020.09.001. Epub 2020 Sep 6. Gait Posture. 2020. PMID: 32927222
Cited by
-
A neuromuscular model of human locomotion combines spinal reflex circuits with voluntary movements.Sci Rep. 2022 May 17;12(1):8189. doi: 10.1038/s41598-022-11102-1. Sci Rep. 2022. PMID: 35581211 Free PMC article.
-
Medial gastrocnemius structure and gait kinetics in spastic cerebral palsy and typically developing children: A cross-sectional study.Medicine (Baltimore). 2018 May;97(21):e10776. doi: 10.1097/MD.0000000000010776. Medicine (Baltimore). 2018. PMID: 29794756 Free PMC article.
-
Number of synergies impacts sensitivity of gait to weakness and contracture.J Biomech. 2022 Mar;134:111012. doi: 10.1016/j.jbiomech.2022.111012. Epub 2022 Feb 18. J Biomech. 2022. PMID: 35219146 Free PMC article.
-
A new strength assessment to evaluate the association between muscle weakness and gait pathology in children with cerebral palsy.PLoS One. 2018 Jan 11;13(1):e0191097. doi: 10.1371/journal.pone.0191097. eCollection 2018. PLoS One. 2018. PMID: 29324873 Free PMC article.
-
Hammering Does Not Fit Fitts' Law.Front Comput Neurosci. 2017 May 29;11:45. doi: 10.3389/fncom.2017.00045. eCollection 2017. Front Comput Neurosci. 2017. PMID: 28611619 Free PMC article.
References
-
- Anderson FC, Pandy MG. A Dynamic Optimization Solution for Vertical Jumping in Three Dimensions. Comput Methods Biomech Biomed Engin. 1999;2:201–231. - PubMed
-
- Blundell SW, Shepherd RB, Dean CM, Adams RD, Cahill BM. Functional strength training in cerebral palsy: a pilot study of a group circuit training class for children aged 4-8 years. Clin Rehabil. 2003;17:48–57. - PubMed
-
- Burden RL, Faires JD, editors. Numerical analysis. Prindle, Weber & Schmidt; Boston, Mass: 1985. 2.1 The Bisection Algorithm; pp. x–676.
-
- Damiano DL, Kelly LE, Vaughn CL. Effects of quadriceps femoris muscle strengthening on crouch gait in children with spastic diplegia. Phys Ther. 1995a;75:658–67. discussion 668-71. - PubMed
