

Microvolt-level T-wave alternans determination using the spectral method in patients with QT prolongation: value of adjusting the T-wave window
- PMID: 22960166
- PMCID: PMC3483387
- DOI: 10.1016/j.jelectrocard.2012.07.007
Microvolt-level T-wave alternans determination using the spectral method in patients with QT prolongation: value of adjusting the T-wave window
Abstract
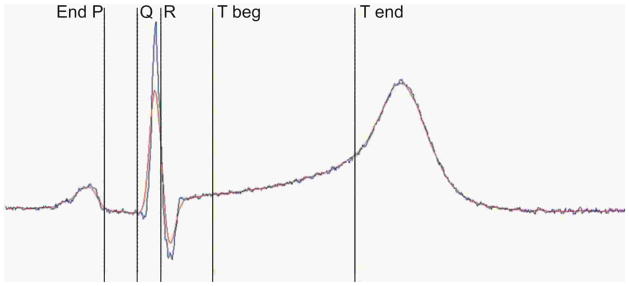
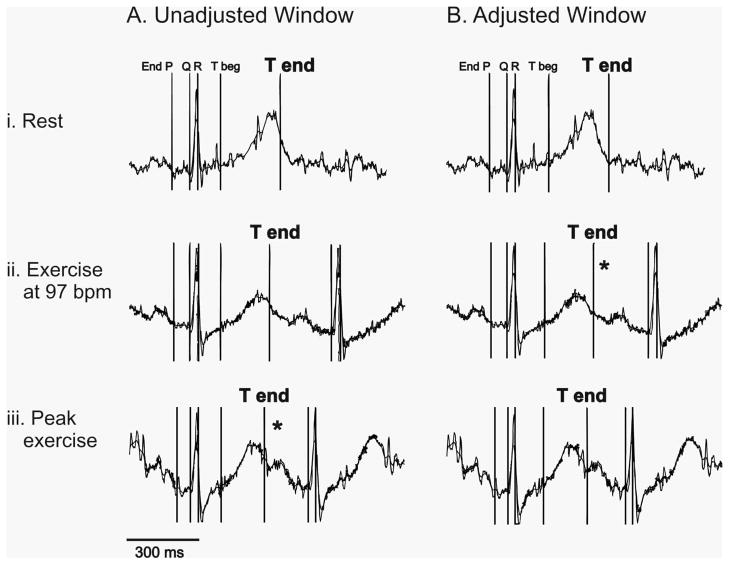
Background: Microvolt-level T-wave alternans (MTWA) measured by the spectral method is a useful risk predictor for sudden cardiac death because of its high negative predictive value. MTWA analysis software selects a segment of the ECG that encompasses the T-wave in most individuals, but may miss the T-wave end in patients with QT prolongation.
Hypotheses: (1) In patients with QT prolongation, adjustment of the T-wave window will increase the sensitivity of MTWA detection. (2) The extent of T-wave window adjustment needed will correspond to the degree of QT prolongation.
Methods: Using data from long-QT syndrome patients, including QTc <0.45 s (normal), 0.45-0.49 s (moderate prolongation), and ≥ 0.50s (severe prolongation), MTWA analysis was performed before and after T-wave window adjustment.
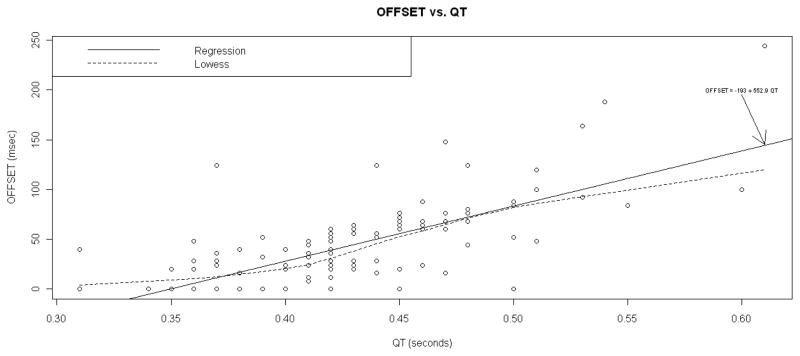
Results: Of 119 patients, 74% required T-wave window adjustment. There was a stronger association between the magnitude of the T-wave offset and the unadjusted QT than between the magnitude of the T-wave offset and QTc (Spearman correlation coefficient 0.690 vs. 0.485 respectively, P<.05). Of 99 initially negative MTWA results, 4 became non-negative after adjustment of the T-wave window (P<.05). All 8 initially positive studies and 12 initially indeterminate studies remained positive and indeterminate, respectively.
Conclusions: T-wave window adjustment can enable detection of abnormal MTWA that otherwise would be classified as "negative" or "normal." Newly developed T-wave window adjustment software may further improve the negative predictive value of MTWA testing and should be validated in a structural heart disease population.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest: this work was funded by a grant (PI: Kaufman) from Cambridge Heart, Inc., who manufacture the equipment used to measure T-wave alternans, and who designed and provided the software modification that allowed us to adjust the T-wave window as described in this paper. Furthermore, one author (Lahn Fendelander) is an employee of Cambridge Heart, Inc.
Figures
Comment in
-
T-wave window adjustment for the determination of microvolt T-wave alternans for all patients?J Electrocardiol. 2013 Jan-Feb;46(1):72. doi: 10.1016/j.jelectrocard.2012.10.003. Epub 2012 Nov 7. J Electrocardiol. 2013. PMID: 23140667 No abstract available.
-
Author's response.J Electrocardiol. 2013 Jan-Feb;46(1):72-3. doi: 10.1016/j.jelectrocard.2012.10.019. Epub 2012 Nov 20. J Electrocardiol. 2013. PMID: 23174502 No abstract available.
References
-
- Pastore JM, Girouard SD, Laurita KR, Akar FG, Rosenbaum DS. Mechanism linking T-wave alternans to the genesis of cardiac fibrillation. Circulation. 1999;99:1385–1394. - PubMed
-
- Hohnloser SH, Ikeda T, Bloomfield DM, Dabbous OH, Cohen RJ. T-wave alternans negative coronary patients with low ejection and benefit from defibrillator implantation. Lancet. 2003;362:125–126. - PubMed
-
- Bloomfield DM, Steinman RC, Namerow PB, Parides M, Davidenko J, Kaufman ES, Shinn T, Curtis A, Fontaine J, Holmes D, Russo A, Tang C, Bigger JT., Jr Microvolt T-wave alternans distinguishes between patients likely and patients not likely to benefit from implanted cardiac defibrillator therapy: a solution to the Multicenter Automatic Defibrillator Implantation Trial (MADIT) II conundrum. Circulation. 2004;110:1885–1889. - PubMed
-
- Schwartz PJ, Malliani A. Electrical alternation of the T-wave: clinical and experimental evidence of its relationship with the sympathetic nervous system and with the long Q-T syndrome. Am Heart J. 1975;89:45–50. - PubMed
-
- Kaufman ES, Priori SG, Napolitano C, Schwartz PJ, Iyengar S, Elston RC, Schnell AH, Gorodeski EZ, Rammohan G, Bahhur NO, Connuck D, Verrilli L, Rosenbaum DS, Brown AM. Electrocardiographic prediction of abnormal genotype in congenital long QT syndrome: experience in 101 related family members. J Cardiovasc Electrophysiol. 2001;12:455–61. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
