

Analysis of reserve capacity and subsequent stenting in a case of subacute occlusion of the internal carotid artery
- PMID: 22960936
- PMCID: PMC3739872
- DOI: 10.1007/s00062-012-0172-z
Analysis of reserve capacity and subsequent stenting in a case of subacute occlusion of the internal carotid artery
Abstract
Introduction: While acute internal carotid artery (ICA) occlusions are increasingly being treated with carotid angioplasty and stenting (CAS), the utility of CAS in subacute stages is unclear.
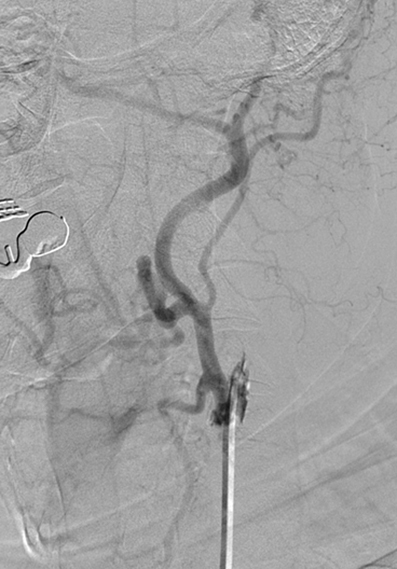
Case Report: A 65-year-old patient with an acute left ICA occlusion and pre-existing occlusion on the right side presented with dysarthria and central right-sided facial palsy. Carbon dioxide (CO2) reactivity within the left hemisphere was markedly reduced. Due to acute deterioration despite maximal conservative therapy CAS was performed 8 days after the initial event with an excellent result and symptoms subsided.
Conclusion: CAS in subacute ICA occlusion is possible. Patients should be selected carefully. Assessment of cerebrovascular CO2 reactivity might provide valuable information.
Figures



Similar articles
-
Follow-up study on in-stent thrombosis after carotid stenting using multidetector CT angiography.Neuroradiology. 2009 Apr;51(4):243-51. doi: 10.1007/s00234-009-0498-7. Epub 2009 Jan 27. Neuroradiology. 2009. PMID: 19172256 Clinical Trial.
-
Stenting and angioplasty of the symptomatic chronically occluded carotid artery.AJNR Am J Neuroradiol. 2007 Jan;28(1):168-71. AJNR Am J Neuroradiol. 2007. PMID: 17213450 Free PMC article.
-
Usefulness of the fusion imaging of 3D-CT and MRA for carotid artery stenting with minimum use of contrast medium in patient with renal dysfunction.Interv Neuroradiol. 2015 Apr;21(2):277-81. doi: 10.1177/1591019915581941. Epub 2015 May 1. Interv Neuroradiol. 2015. PMID: 25934657 Free PMC article.
-
Stenting for Internal Carotid Artery Stenosis Associated with Persistent Primitive Hypoglossal Artery Using Proximal Flow Blockade and Distal Protection System: A Technical Case Report and Literature Review.J Stroke Cerebrovasc Dis. 2016 Jun;25(6):e98-e102. doi: 10.1016/j.jstrokecerebrovasdis.2016.03.026. Epub 2016 Apr 19. J Stroke Cerebrovasc Dis. 2016. PMID: 27105567 Review.
-
What are current preprocedure imaging requirements for carotid artery stenting and carotid endarterectomy: have magnetic resonance angiography and computed tomographic angiography made a difference?Semin Vasc Surg. 2007 Dec;20(4):205-15. doi: 10.1053/j.semvascsurg.2007.10.002. Semin Vasc Surg. 2007. PMID: 18082837 Review.
Cited by
-
Current understanding of chronic total occlusion of the internal carotid artery.Biomed Rep. 2018 Feb;8(2):117-125. doi: 10.3892/br.2017.1033. Epub 2017 Dec 18. Biomed Rep. 2018. PMID: 29435269 Free PMC article.
-
Breath holding for 20 s following extended expiration is a practical, effective and robust standard when measuring cerebrovascular reactivity in healthy adults using BOLD fMRI at 3 T.Neuroimage Rep. 2021 Jun 14;1(2):100021. doi: 10.1016/j.ynirp.2021.100021. eCollection 2021 Jun. Neuroimage Rep. 2021. PMID: 40567865 Free PMC article.
References
-
- O’Hara PJ, Hertzer NR, Beven EG. External carotid revascularization: review of a ten-year experience. J Vasc Surg. 1985;2(5):709–14. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
