

Public health implications of recommendations to individualize glycemic targets in adults with diabetes
- PMID: 22961575
- PMCID: PMC3526201
- DOI: 10.2337/dc11-2344
Public health implications of recommendations to individualize glycemic targets in adults with diabetes
Abstract
Objective: To estimate how many U.S. adults with diabetes would be eligible for individualized A1C targets based on 1) the 2012 American Diabetes Association (ADA) guideline and 2) a published approach for individualized target ranges.
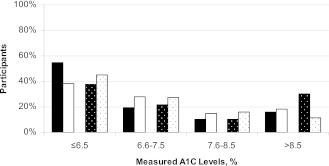
Research design and methods: We studied adults with diabetes ≥20 years of age from the National Health and Nutrition Examination Survey 2007-2008 (n = 757). We assigned A1C targets based on duration, age, diabetes-related complications, and comorbid conditions according to 1) the ADA guideline and 2) a strategy by Ismail-Beigi focused on setting target ranges. We estimated the number and proportion of adults with each A1C target and compared individualized targets to measured levels.
Results: Using ADA guideline recommendations, 31% (95% CI 27-34%) of the U.S. adult diabetes population would have recommended A1C targets of <7.0%, and 69% (95% CI 66-73%) would have A1C targets less stringent than <7.0%. Using the Ismail-Beigi strategy, 56% (51-61%) would have an A1C target of ≤7.0%, and 44% (39-49%) would have A1C targets less stringent than <7.0%. If a universal A1C <7.0% target were applied, 47% (41-54%) of adults with diabetes would have inadequate glycemic control; this proportion declined to 30% (26-36%) with the ADA guideline and 31% (27-36%) with the Ismail-Beigi strategy.
Conclusions: Using individualized glycemic targets, about half of U.S. adults with diabetes would have recommended A1C targets of ≥7.0% but one-third would still be considered inadequately controlled. Diabetes research and performance measurement goals will need to be revised in order to encourage the individualization of glycemic targets.
Figures
References
-
- Brown AF, Mangione CM, Saliba D, Sarkisian CA, California Healthcare Foundation/American Geriatrics Society Panel on Improving Care for Elders with Diabetes Guidelines for improving the care of the older person with diabetes mellitus. J Am Geriatr Soc 2003;51(Suppl. Guidelines):S265–S280 - PubMed
-
- Handelsman Y, Mechanick JI, Blonde L, et al. AACE Task Force for Developing Diabetes Comprehensive Care Plan American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for developing a diabetes mellitus comprehensive care plan. Endocr Pract 2011;17(Suppl. 2):1–53 - PubMed
-
- Management of Diabetes Mellitus Update Working Group VA/DoD Clinical Practice Guideline for the Management of Diabetes Mellitus. Version 4.0. Washington, DC, Veterans Health Administration and Department of Defense, 2010
-
- Qaseem A, Vijan S, Snow V, Cross JT, Weiss KB, Owens DK, Clinical Efficacy Assessment Subcommittee of the American College of Physicians Glycemic control and type 2 diabetes mellitus: the optimal hemoglobin A1c targets. A guidance statement from the American College of Physicians. Ann Intern Med 2007;147:417–422 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
