

Insights from a novel model of slow-transit constipation generated by partial outlet obstruction in the murine large intestine
- PMID: 22961801
- PMCID: PMC3517665
- DOI: 10.1152/ajpgi.00238.2012
Insights from a novel model of slow-transit constipation generated by partial outlet obstruction in the murine large intestine
Abstract
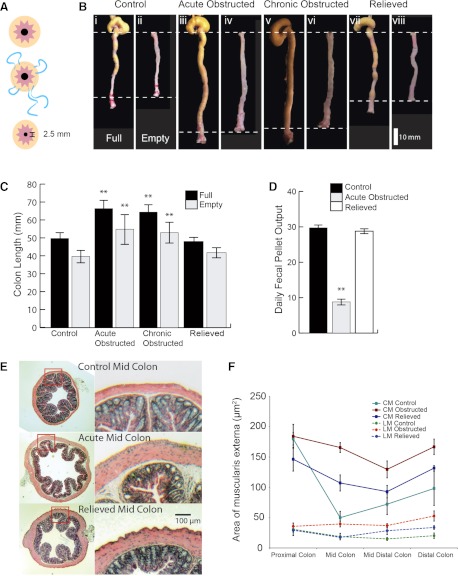
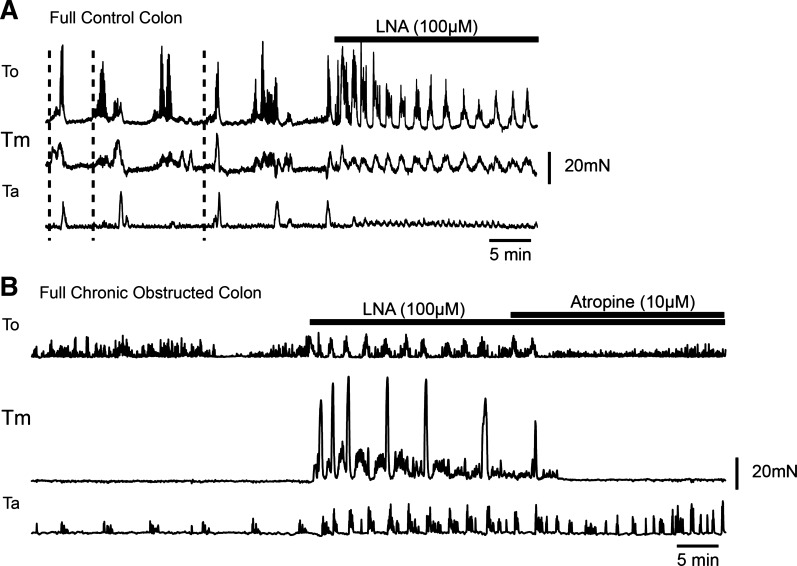
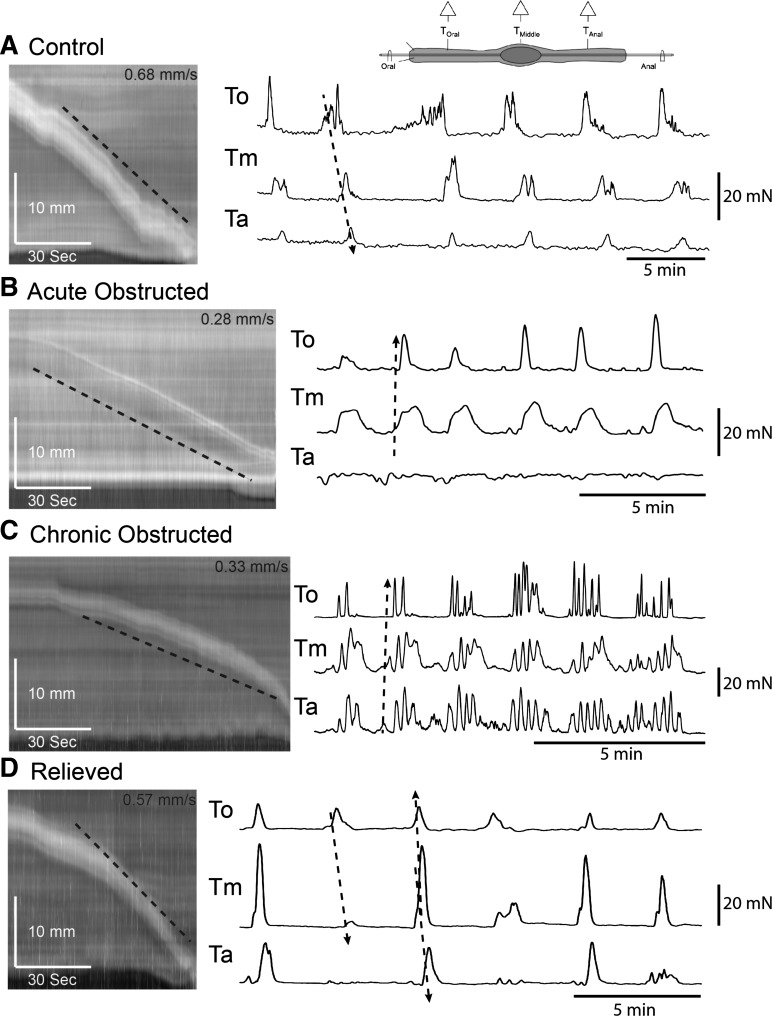
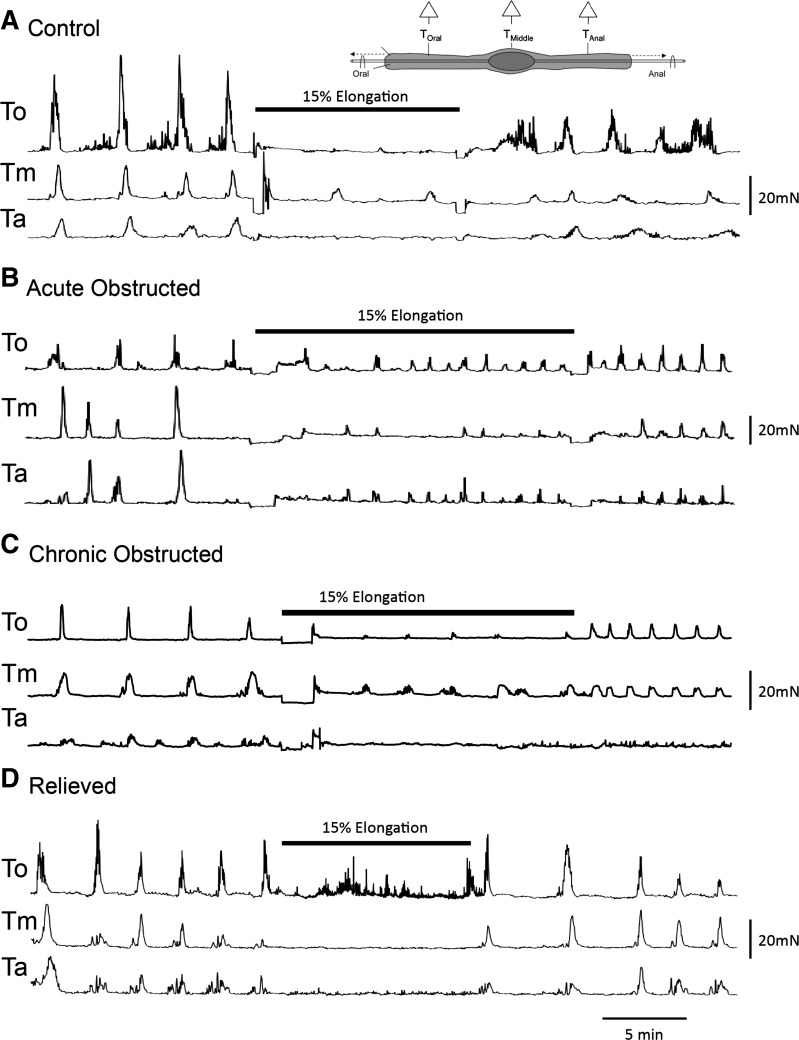
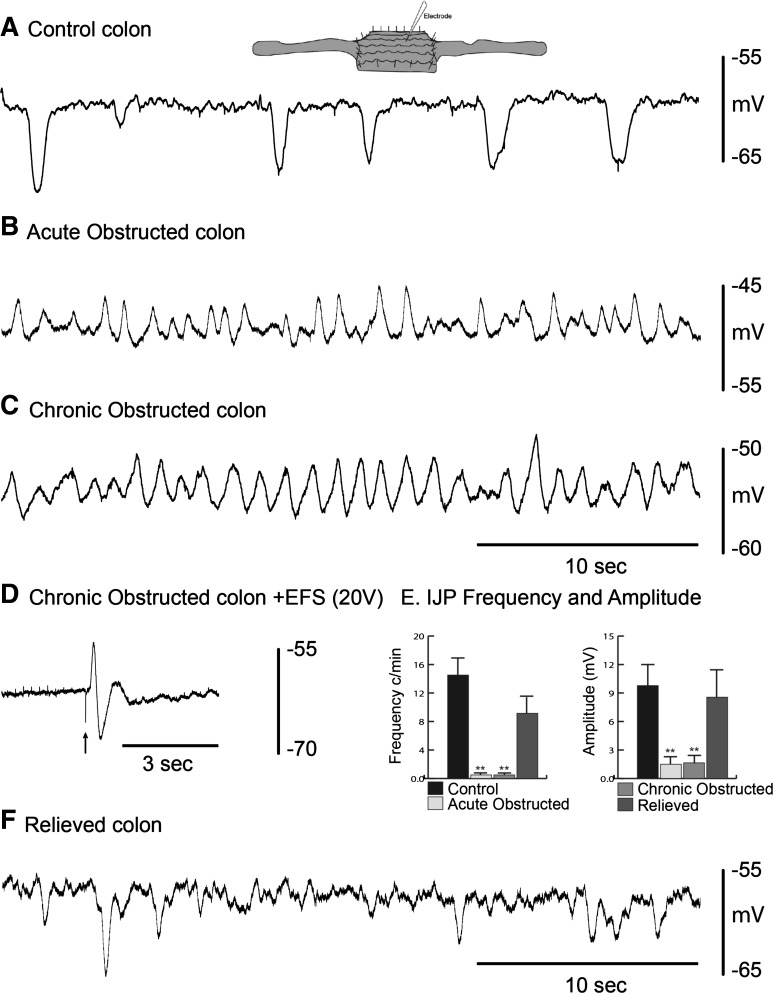
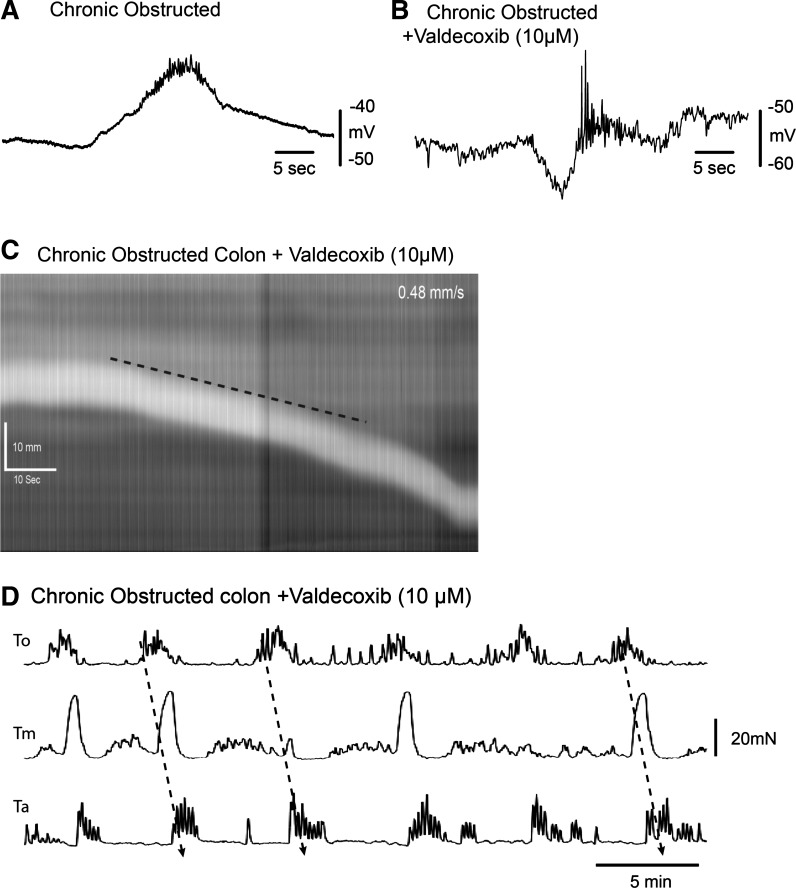
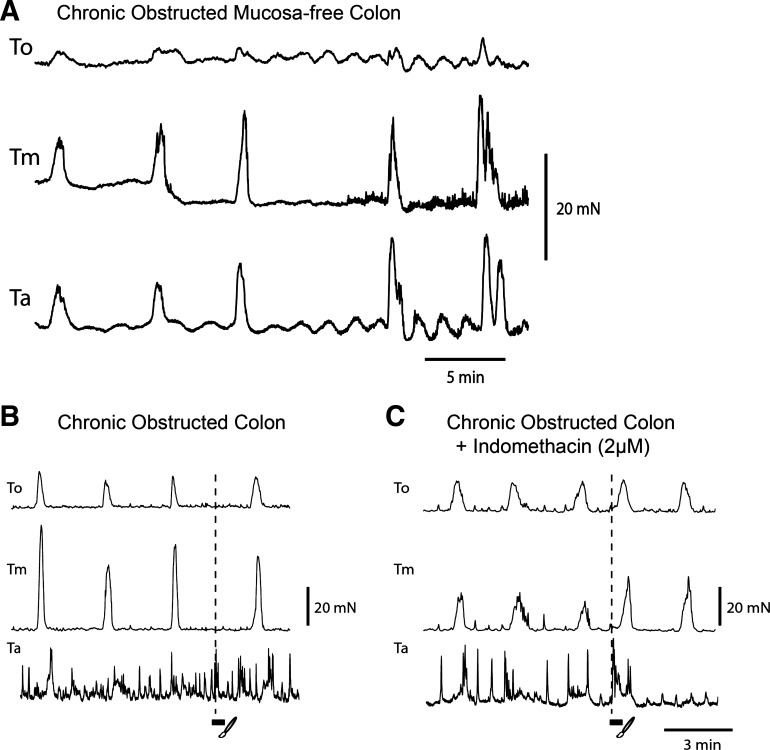
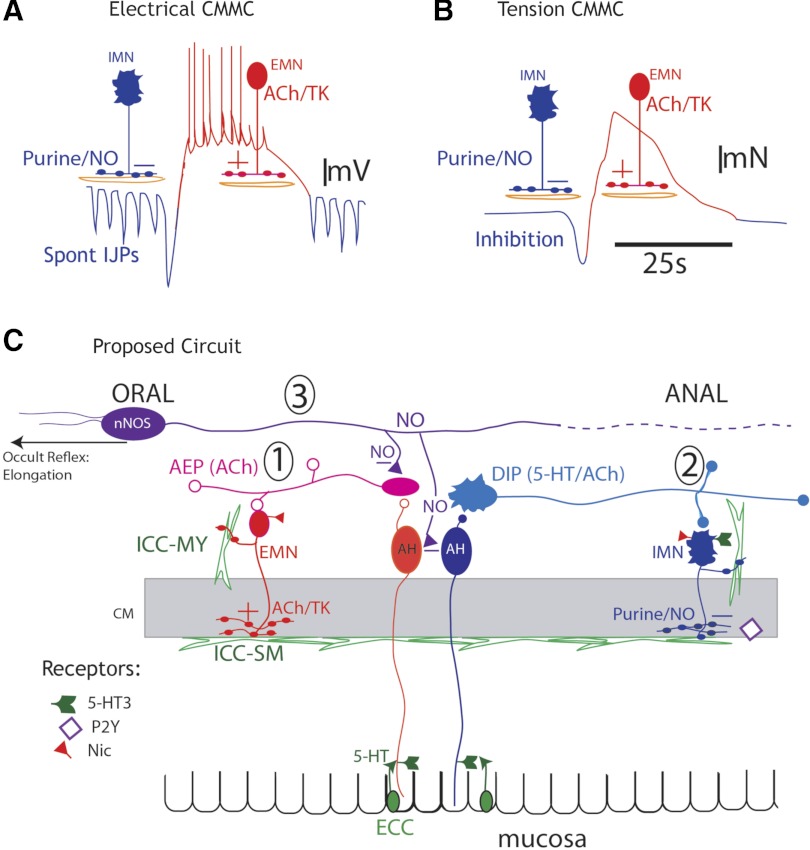
The mechanisms underlying slow-transit constipation (STC) are unclear. In 50% of patients with STC, some form of outlet obstruction has been reported; also an elongated colon has been linked to patients with STC. Our aims were 1) to develop a murine model of STC induced by partial outlet obstruction and 2) to determine whether this leads to colonic elongation and, consequently, activation of the inhibitory "occult reflex," which may contribute to STC in humans. Using a purse-string suture, we physically reduced the maximal anal sphincter opening in C57BL/6 mice. After 4 days, the mice were euthanized (acutely obstructed), the suture was removed (relieved), or the suture was removed and replaced repeatedly (chronically obstructed, over 24-31 days). In partially obstructed mice, we observed increased cyclooxygenase (COX)-2 levels in muscularis and mucosa, an elongated impacted large bowel, slowed transit, nonpropagating colonic migrating motor complexes (CMMCs), a lack of mucosal reflexes, a depolarized circular muscle with slow-wave activity due to a lack of spontaneous inhibitory junction potentials, muscle hypertrophy, and CMMCs in mucosa-free preparations. Elongation of the empty obstructed colon produced a pronounced occult reflex. Removal of the obstruction or addition of a COX-2 antagonist (in vitro and in vivo) restored membrane potential, spontaneous inhibitory junction potentials, CMMC propagation, and mucosal reflexes. We conclude that partial outlet obstruction increases COX-2 leading to a hyperexcitable colon. This hyperexcitability is largely due to suppression of only descending inhibitory nerve pathways by prostaglandins. The upregulation of motility is suppressed by the occult reflex activated by colonic elongation.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials