

Central QCT reveals lower volumetric BMD and stiffness in premenopausal women with idiopathic osteoporosis, regardless of fracture history
- PMID: 22962425
- PMCID: PMC3485589
- DOI: 10.1210/jc.2012-2099
Central QCT reveals lower volumetric BMD and stiffness in premenopausal women with idiopathic osteoporosis, regardless of fracture history
Abstract
Context: Idiopathic osteoporosis (IOP) affects otherwise healthy young individuals with intact gonadal function and no secondary cause of bone fragility. In premenopausal women with IOP, a low trauma fracture is evidence of impaired bone quality and strength. The extent to which low bone mineral density (BMD) by dual-energy x-ray absorptiometry (DXA) reflects low volumetric BMD, bone microstructure, and strength is uncertain in the absence of low trauma fracture.
Objective: The objective of the study was to compare three-dimensional volumetric BMD and bone stiffness in premenopausal women with IOP based on fracture history, those with idiopathic low BMD (Z score ≤ -2.0) and no low trauma fracture, and normal age-matched controls.
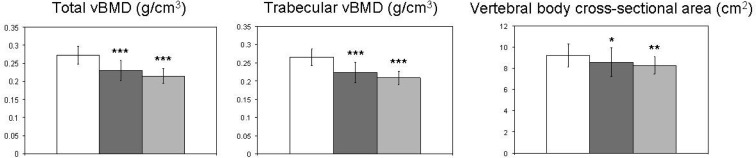
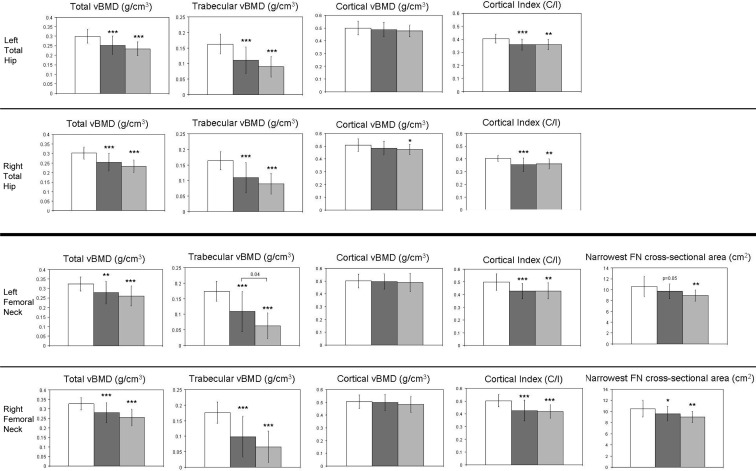
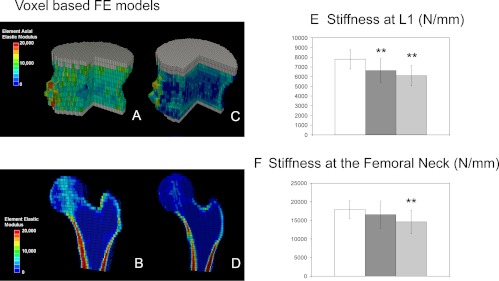
Design: We measured volumetric BMD and bone geometry by central quantitative computed tomography (cQCT) scans of the spine and hip and estimated bone stiffness by finite element analysis of cQCT data sets in 32 premenopausal women with IOP, 12 with idiopathic low BMD, and 34 controls.
Results: Subjects had comparable decreases in total and trabecular volumetric BMD, cortical thickness, and whole-bone stiffness compared with controls, regardless of fracture history. These differences remained significant after controlling for age, body mass index, and bone size. The positive predictive values of a DXA Z score of -2.0 or less for a cQCT volumetric BMD Z score of -2.0 or less were 95% at the lumbar spine, 90% at the total hip, and 86% at the femoral neck.
Conclusion: Women with idiopathic low BMD alone and those with low trauma fractures had comparable deficits in bone mass, structure, and stiffness. Low areal BMD by DXA is fairly accurate for predicting low volumetric BMD by cQCT. These results are consistent with three-dimensional bone imaging at the iliac crest, radius, and tibia in premenopausal IOP and suggest that the term osteoporosis may be appropriate in women with Z scores below -2.0, whether or not there is a history of fracture.
Figures
References
-
- Adams J, Bishop N. 2008. DXA in adults and children. In: Rosen CJ, ed. Primer on the metabolic bone diseases and disorders of mineral metabolism. Chap 29 Washington, DC: American Society for Bone and Mineral Research; 152–158
-
- Cohen A, Shane E. 2008. Premenopausal osteoporosis. In: Rosen CJ, ed. Primer on the metabolic bone diseases and other disorders of bone and mineral metabolism. Washington, DC: American Society for Bone and Mineral Research; 289–293
-
- Kahn AA, Syed Z. 2004. Bone densitometry in premenopausal women: synthesis and review. J Clin Densitom 7:85–92 - PubMed
-
- Gourlay ML, Brown SA. 2004. Clinical considerations in premenopausal osteoporosis. Arch Intern Med 164:603–614 - PubMed
-
- Lewiecki EM. 2004. Low bone mineral density in premenopausal women. South Med J 97:544–550 - PubMed
