

Evaluation of supply-side initiatives to improve access to coronary bypass surgery
- PMID: 22963283
- PMCID: PMC3515401
- DOI: 10.1186/1472-6963-12-311
Evaluation of supply-side initiatives to improve access to coronary bypass surgery
Abstract
Background: Guided by the evidence that delaying coronary revascularization may lead to symptom worsening and poorer clinical outcomes, expansion in cardiac surgery capacity has been recommended in Canada. Provincial governments started providing one-time and recurring increases in budgets for additional open heart surgeries to reduce waiting times. We sought to determine whether the year of decision to proceed with non-emergency coronary bypass surgery had an effect on time to surgery.
Methods: Using records from a population-based registry, we studied times between decision to operate and the procedure itself. We estimated changes in the length of time that patients had to wait for non-emergency operation over 14 calendar periods that included several years when supplementary funding was available. We studied waiting times separately for patients who access surgery through a wait list and through direct admission.
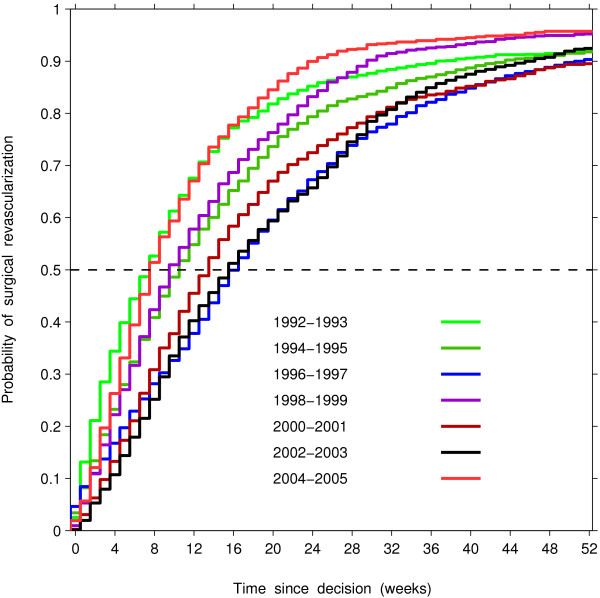
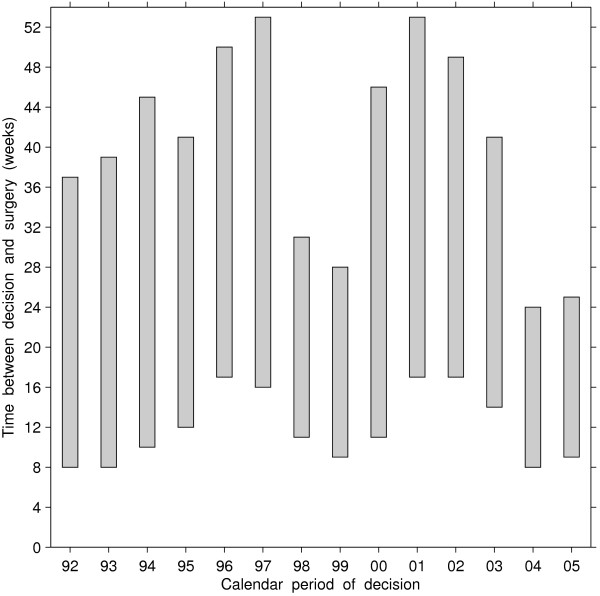
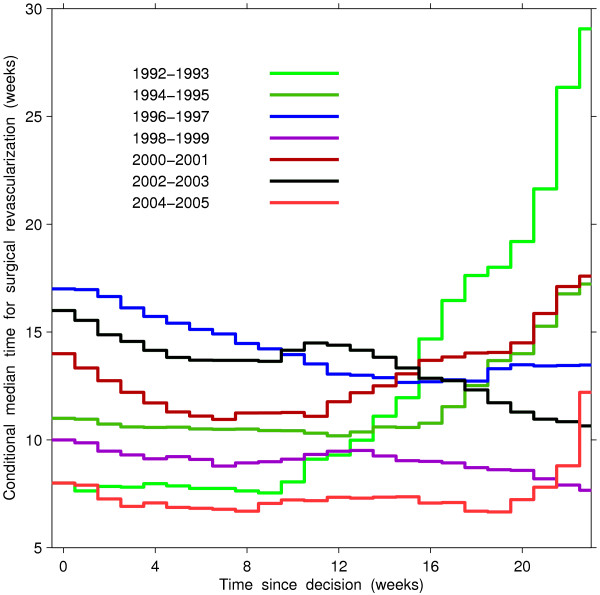
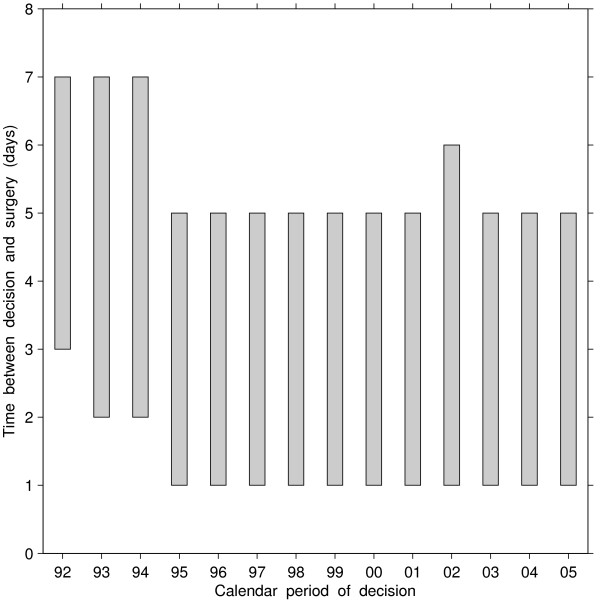
Results: During two periods when supplementary funding was available, 1998-1999 and 2004-2005, the weekly rate of undergoing surgery from a wait list was, respectively, 50% and 90% higher than in 1996-1997, the period with the longest waiting times. We also observed a reduction in the difference between 90th and 50th percentiles of the waiting-time distributions. Forty percent of patients in the 1998, 1999, 2004 and 2005 cohorts (years when supplementary funding was provided) underwent surgery within 16 to 20 weeks following the median waiting time, while it took between 27 and 37 weeks for the cohorts registered in the years when supplementary funding was not available. Times between decision and surgery were shorter for direct admissions than for wait-listed patients. Among patients who were directly admitted to hospital, time between decision and surgery was longest in 1992-1993 and then has been steadily decreasing through the late nineties. The rate of surgery among these patients was the highest in 1998-1999, and has not changed afterwards, even for years when supplementary funding was provided.
Conclusions: Waiting times for non-emergency coronary bypass surgery shortened after supplementary funding was granted to increase volume of cardiac surgical care in a health system with publicly-funded universal coverage for the procedure. The effect of the supplementary funding was not uniform for patients that access the services through wait lists and through direct admission.
Figures
References
-
- Rihal CS, Raco DL, Gersh BJ, Yusuf S. Indications for coronary artery bypass surgery and percutaneous coronary intervention in chronic stable angina: review of the evidence and methodological considerations. Circulation. 2003;108(20):2439–2445. doi: 10.1161/01.CIR.0000094405.21583.7C. - DOI - PubMed
-
- Fierlbeck K. Health Care in Canada: A Citizen’s Guide to Policy and Politics. Toronto: University of Toronto Press; chap. Funding Health Care; 2011: 3–43.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
