

Administration of cardiac stem cells in patients with ischemic cardiomyopathy: the SCIPIO trial: surgical aspects and interim analysis of myocardial function and viability by magnetic resonance
- PMID: 22965994
- PMCID: PMC3448934
- DOI: 10.1161/CIRCULATIONAHA.112.092627
Administration of cardiac stem cells in patients with ischemic cardiomyopathy: the SCIPIO trial: surgical aspects and interim analysis of myocardial function and viability by magnetic resonance
Abstract
Background: SCIPIO is a first-in-human, phase 1, randomized, open-label trial of autologous c-kit(+) cardiac stem cells (CSCs) in patients with heart failure of ischemic etiology undergoing coronary artery bypass grafting (CABG). In the present study, we report the surgical aspects and interim cardiac magnetic resonance (CMR) results.
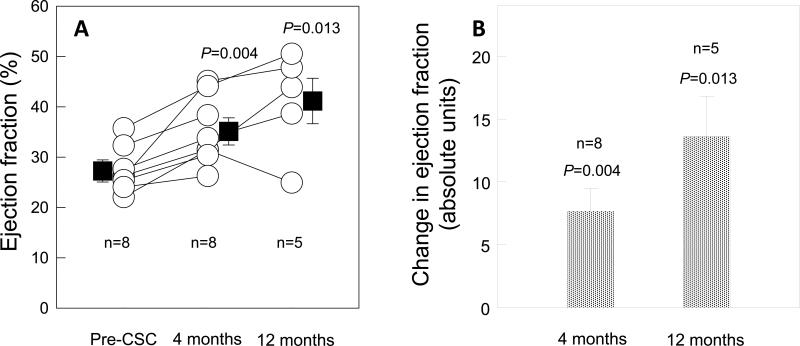
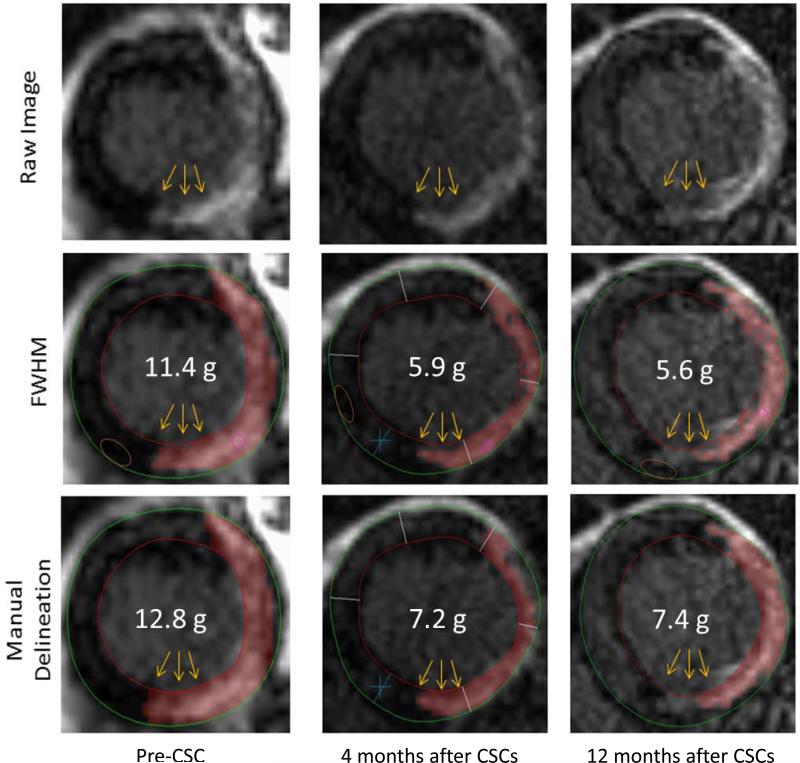
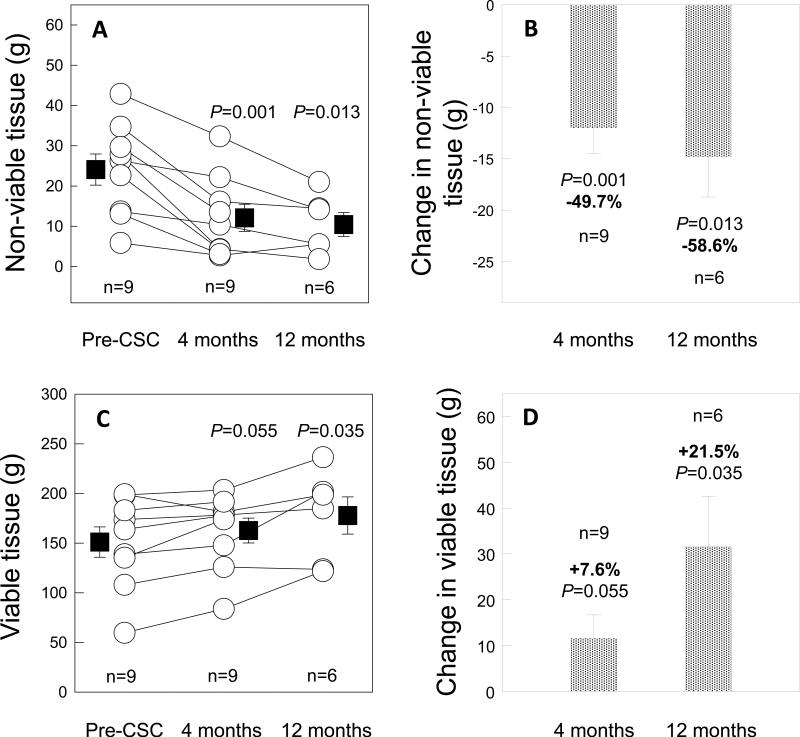
Methods and results: A total of 33 patients (20 CSC-treated and 13 control subjects) met final eligibility criteria and were enrolled in SCIPIO. CSCs were isolated from the right atrial appendage harvested and processed during surgery. Harvesting did not affect cardiopulmonary bypass, cross-clamp, or surgical times. In CSC-treated patients, CMR showed a marked increase in both LVEF (from 27.5 ± 1.6% to 35.1 ± 2.4% [P=0.004, n=8] and 41.2 ± 4.5% [P=0.013, n=5] at 4 and 12 months after CSC infusion, respectively) and regional EF in the CSC-infused territory. Infarct size (late gadolinium enhancement) decreased after CSC infusion (by manual delineation: -6.9 ± 1.5 g [-22.7%] at 4 months [P=0.002, n=9] and -9.8 ± 3.5 g [-30.2%] at 12 months [P=0.039, n=6]). LV nonviable mass decreased even more (-11.9 ± 2.5 g [-49.7%] at 4 months [P=0.001] and -14.7 ± 3.9 g [-58.6%] at 12 months [P=0.013]), whereas LV viable mass increased (+11.6 ± 5.1 g at 4 months after CSC infusion [P=0.055] and +31.5 ± 11.0 g at 12 months [P=0.035]).
Conclusions: Isolation of CSCs from cardiac tissue obtained in the operating room is feasible and does not alter practices during CABG surgery. CMR shows that CSC infusion produces a striking improvement in both global and regional LV function, a reduction in infarct size, and an increase in viable tissue that persist at least 1 year and are consistent with cardiac regeneration.
Clinical trial registration: This study is registered with clinicaltrials.gov, trial number NCT00474461.
Figures



References
-
- Roger VL, Go AS, Lloyd-Jones DM, Adams RJ, Berry JD, Brown TM, Carnethon MR, Dai S, de Simone G, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Greenlund KJ, Hailpern SM, Heit JA, Ho PM, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, McDermott MM, Meigs JB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Rosamond WD, Sorlie PD, Stafford RS, Turan TN, Turner MB, Wong ND, Wylie-Rosett J, American Heart Association Statistics C. Stroke Statistics S Heart disease and stroke statistics--2011 update: A report from the american heart association. Circulation. 2011;123:e18–e209. - PMC - PubMed
-
- Baldasseroni S, Opasich C, Gorini M, Lucci D, Marchionni N, Marini M, Campana C, Perini G, Deorsola A, Masotti G, Tavazzi L, Maggioni AP. Left bundle-branch block is associated with increased 1-year sudden and total mortality rate in 5517 outpatients with congestive heart failure: A report from the italian network on congestive heart failure. American heart journal. 2002;143:398–405. - PubMed
-
- Kalogeropoulos A, Georgiopoulou V, Kritchevsky SB, Psaty BM, Smith NL, Newman AB, Rodondi N, Satterfield S, Bauer DC, Bibbins-Domingo K, Smith AL, Wilson PW, Vasan RS, Harris TB, Butler J. Epidemiology of incident heart failure in a contemporary elderly cohort: The health, aging, and body composition study. Archives of internal medicine. 2009;169:708–715. - PMC - PubMed
-
- He J, Ogden LG, Bazzano LA, Vupputuri S, Loria C, Whelton PK. Risk factors for congestive heart failure in us men and women: Nhanes i epidemiologic follow-up study. Archives of internal medicine. 2001;161:996–1002. - PubMed
-
- Abdel-Latif A, Bolli R, Tleyjeh IM, Montori VM, Perin EC, Hornung CA, Zuba-Surma EK, Al-Mallah M, Dawn B. Adult bone marrow-derived cells for cardiac repair: A systematic review and meta-analysis. Arch Intern Med. 2007;167:989–997. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
