

Imaging features of superficial and deep fibromatoses in the adult population
- PMID: 22966216
- PMCID: PMC3395298
- DOI: 10.1155/2012/215810
Imaging features of superficial and deep fibromatoses in the adult population
Abstract
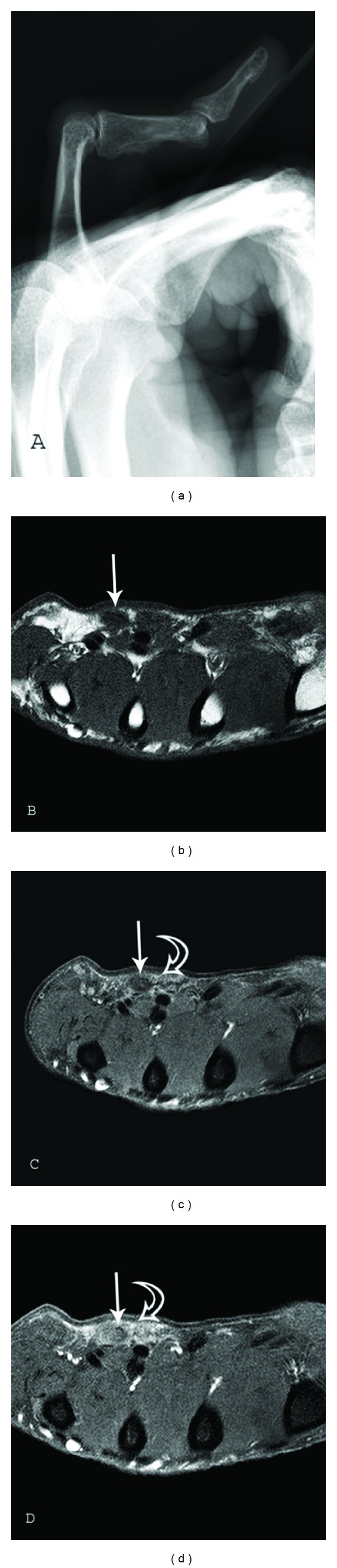
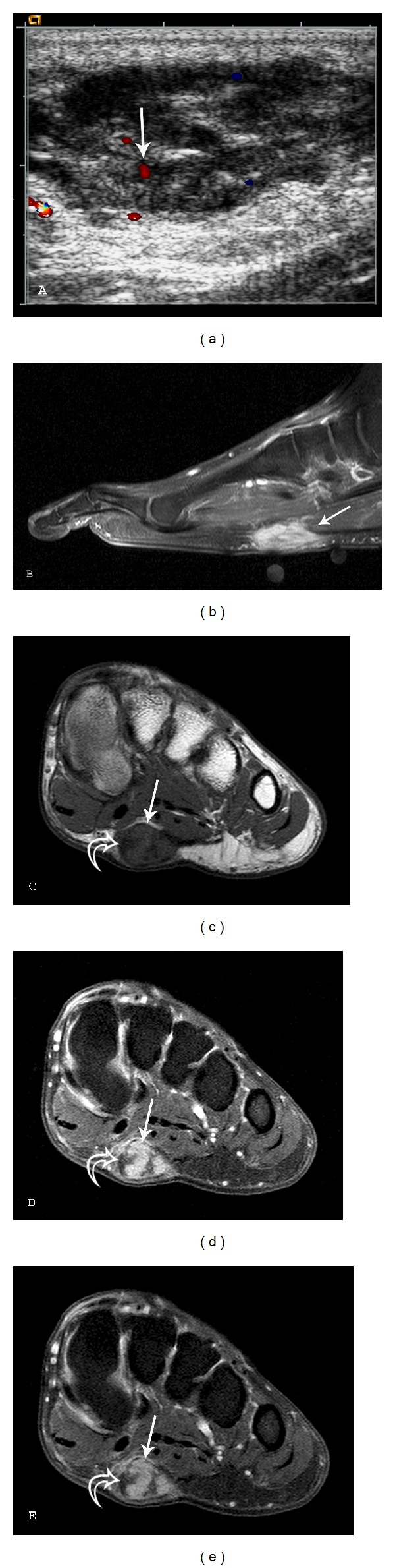
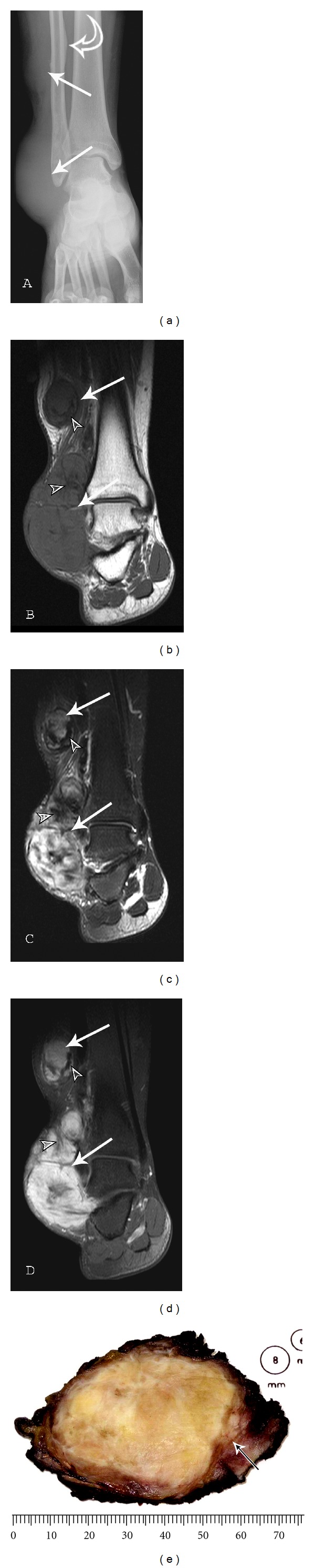
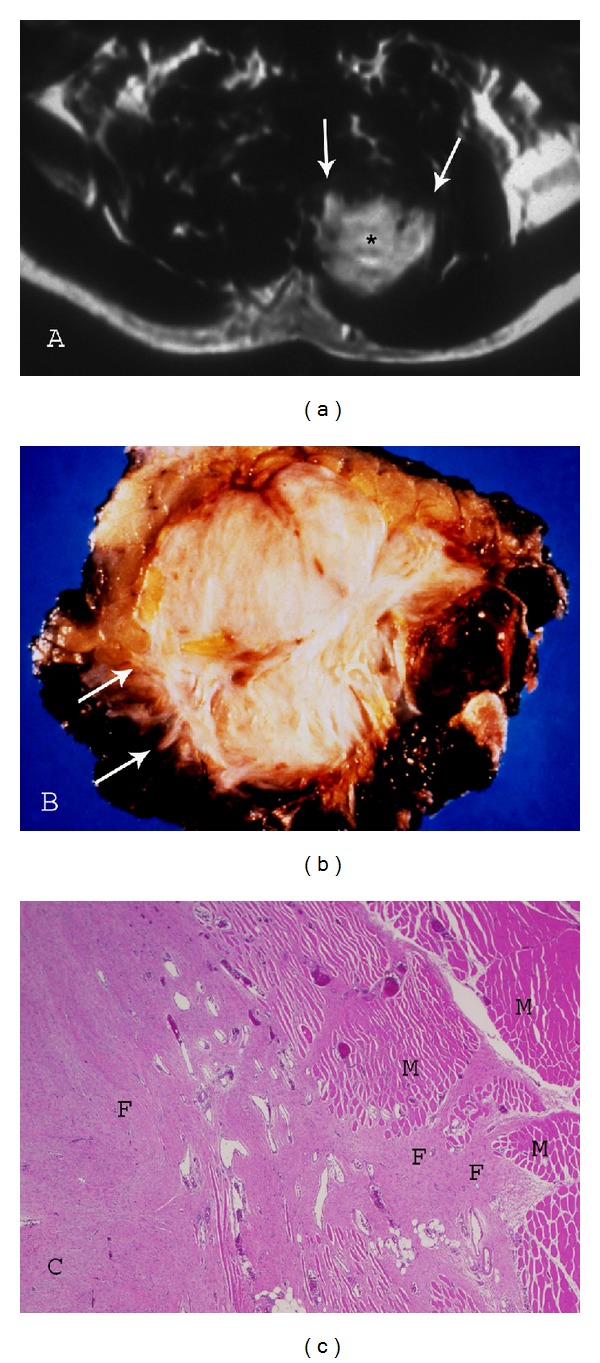
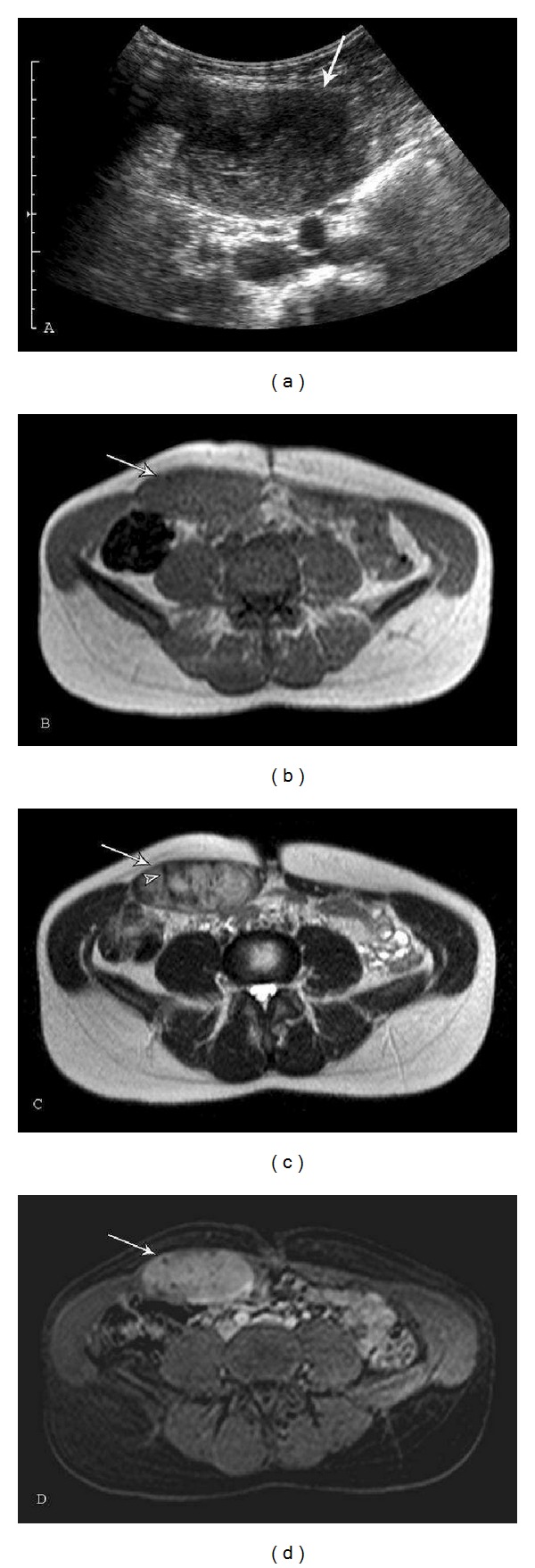
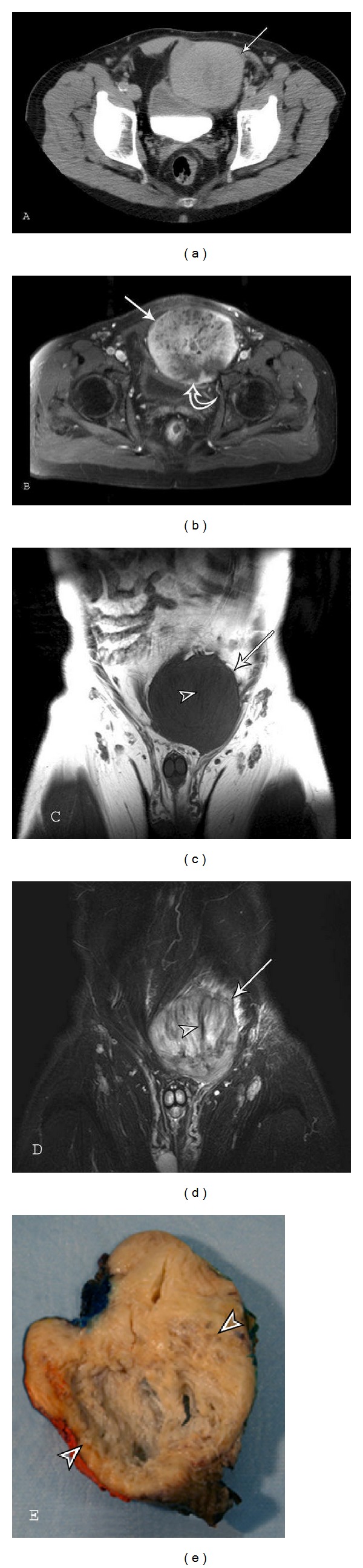
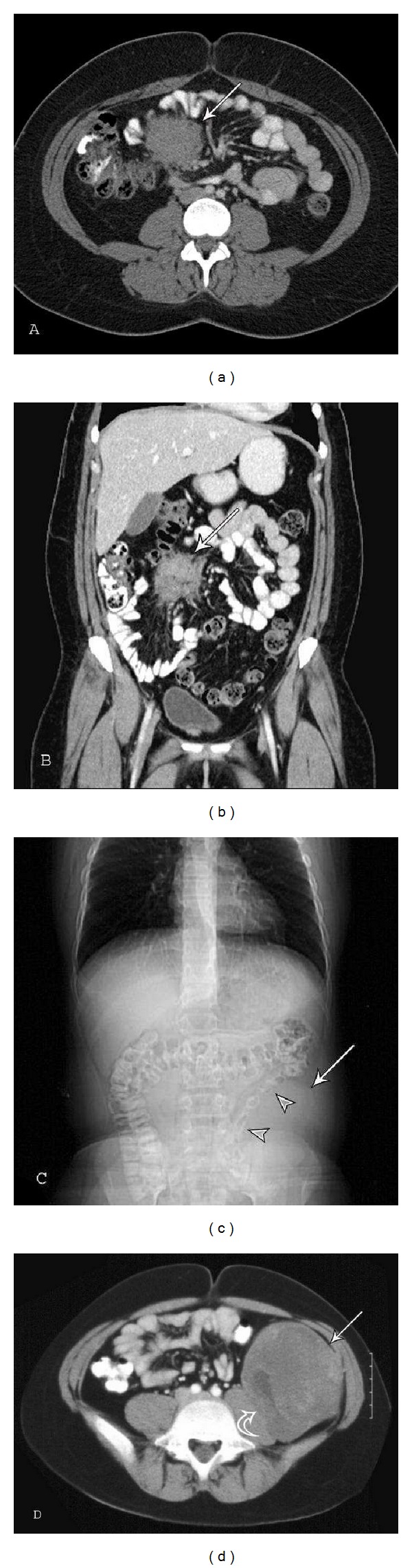
The fibromatoses are a group of benign fibroblastic proliferations that vary from benign to intermediate in biological behavior. This article will discuss imaging characteristics and patient demographics of the adult type superficial (fascial) and deep (musculoaponeurotic) fibromatoses. The imaging appearance of these lesions can be characteristic (particularly when using magnetic resonance imaging). Palmar fibromatosis demonstrates multiple nodular or band-like soft tissue masses arising from the proximal palmar aponeurosis and extending along the subcutaneous tissues of the finger in parallel to the flexor tendons. T1 and T2-weighted signal intensity can vary from low (higher collagen) to intermediate (higher cellularity), similar to the other fibromatoses. Plantar fibromatosis manifests as superficial lesions along the deep plantar aponeurosis, which typically blend with the adjacent plantar musculature. Linear tails of extension ("fascial tail sign") along the aponeurosis are frequent. Extraabdominal and abdominal wall fibromatosis often appear as a heterogeneous lesion with low signal intensity bands on all pulse sequences and linear fascial extensions ("fascial tail" sign) with MR imaging. Mesenteric fibromatosis usually demonstrates a soft tissue density on CT with radiating strands projecting into the adjacent mesenteric fat. When imaging is combined with patient demographics, a diagnosis can frequently be obtained.
Figures





Similar articles
-
Imaging of musculoskeletal fibromatosis.Radiographics. 2001 May-Jun;21(3):585-600. doi: 10.1148/radiographics.21.3.g01ma21585. Radiographics. 2001. PMID: 11353108 Review.
-
From the archives of the AFIP: musculoskeletal fibromatoses: radiologic-pathologic correlation.Radiographics. 2009 Nov;29(7):2143-73. doi: 10.1148/rg.297095138. Radiographics. 2009. PMID: 19926768
-
MR imaging in fibromatosis: results in 26 patients with pathologic correlation.AJR Am J Roentgenol. 1991 Mar;156(3):539-42. doi: 10.2214/ajr.156.3.1899752. AJR Am J Roentgenol. 1991. PMID: 1899752
-
Multi-parametric (mp) MRI for the diagnosis of abdominal wall desmoid tumors.Eur J Radiol. 2017 Jul;92:103-110. doi: 10.1016/j.ejrad.2017.04.010. Epub 2017 Apr 17. Eur J Radiol. 2017. PMID: 28624006
-
Clinical features and management of superficial fibromatoses.J Dtsch Dermatol Ges. 2019 Apr;17(4):393-397. doi: 10.1111/ddg.13808. Epub 2019 Mar 13. J Dtsch Dermatol Ges. 2019. PMID: 30865379 Review.
Cited by
-
Soft Tissue Masses of the Hand: A Review of Clinical Presentation and Imaging Features.Curr Oncol. 2023 Feb 7;30(2):2032-2048. doi: 10.3390/curroncol30020158. Curr Oncol. 2023. PMID: 36826119 Free PMC article. Review.
-
Preoperative Factors Associated with Infiltrative Histologic Growth Patterns in Extremity Soft Tissue Sarcoma.Sarcoma. 2017;2017:5419394. doi: 10.1155/2017/5419394. Epub 2017 Jul 20. Sarcoma. 2017. PMID: 28808411 Free PMC article.
-
An update on the management of sporadic desmoid-type fibromatosis: a European Consensus Initiative between Sarcoma PAtients EuroNet (SPAEN) and European Organization for Research and Treatment of Cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG).Ann Oncol. 2017 Oct 1;28(10):2399-2408. doi: 10.1093/annonc/mdx323. Ann Oncol. 2017. PMID: 28961825 Free PMC article. Review.
-
Giant fibroepithelial polyp of the thigh and retroperitoneal fibromatosis in a young woman: a rare case.Skeletal Radiol. 2018 Sep;47(9):1299-1304. doi: 10.1007/s00256-018-2904-x. Epub 2018 Feb 27. Skeletal Radiol. 2018. PMID: 29487969
-
Differentiation of intra-abdominal desmoid tumor from peritoneal seeding based on CT and/or 18F-FDG PET-CT in patients with history of cancer surgery.Abdom Radiol (NY). 2020 Sep;45(9):2647-2655. doi: 10.1007/s00261-020-02620-5. Epub 2020 Jun 19. Abdom Radiol (NY). 2020. PMID: 32562052
References
-
- Weiss SW, Goldblum JR, Enzinger FM. Fibromatoses. In: Weiss SW, Goldblum JR, editors. Enzinger and Weiss' Soft Tissue Tumors. Philadelphia, Pa, USA: Mosby Elsevier; 2008. pp. 227–228.
-
- Fletcher CDM, Krishnan Unni K, Mertens F, editors. Pathology and Genetics of Tumours of Soft Tissue and Bone (IARC WHO Classification of Tumours) 3rd edition 2006.
-
- Murphey MD, Ruble CM, Tyszko SM, Zbojniewicz AM, Potter BK, Miettinen M. From the archives of the AFIP: musculoskeletal fibromatoses: radiologic-pathologic correlation. Radiographics. 2009;29(7):2143–2176. - PubMed
-
- Yost J, Winters T, Fett HC. Dupuytren’s contracture: a statistical study. The American Journal of Surgery. 1955;90(4):568–571. - PubMed
-
- Kempson RL, Armed Forces Institute of Pathology (U.S.), Universities Associated for Research and Education in Pathology . Tumors of the Soft Tissues. Atlas of Tumor Pathology. 3rd edition. Washington, DC, USA: Armed Forces Institute of Pathology; 2001.
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
