

Giant serous microcystic adenoma of the pancreas safely resected after preoperative arterial embolization
- PMID: 22966391
- PMCID: PMC3436451
- DOI: 10.3892/ol_00000148
Giant serous microcystic adenoma of the pancreas safely resected after preoperative arterial embolization
Abstract
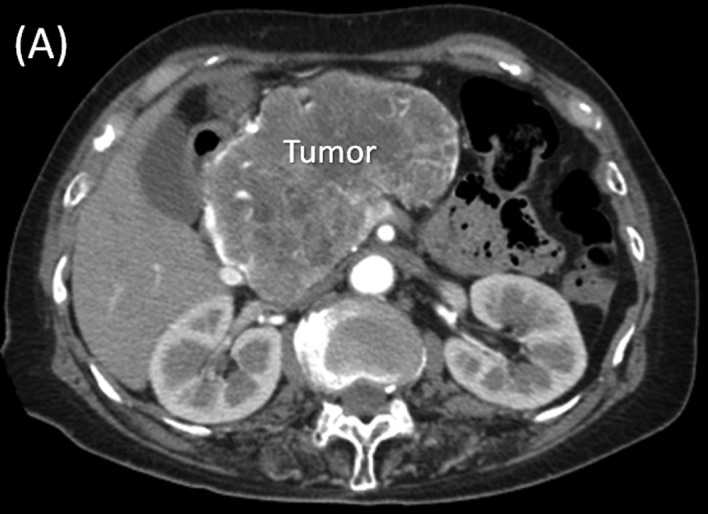
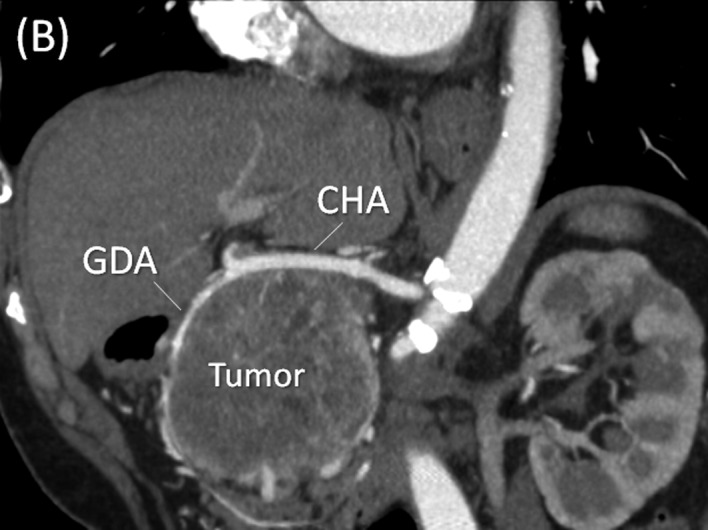
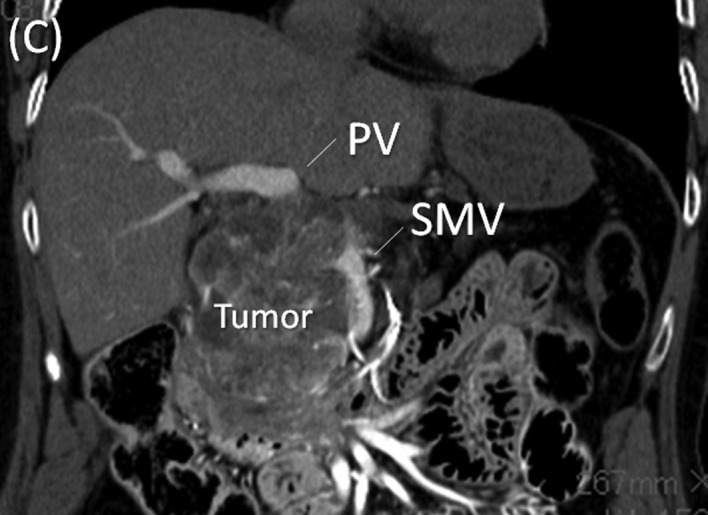
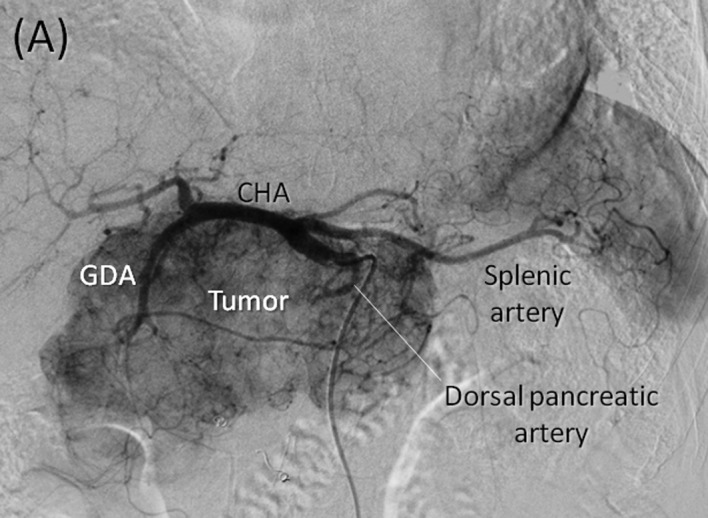
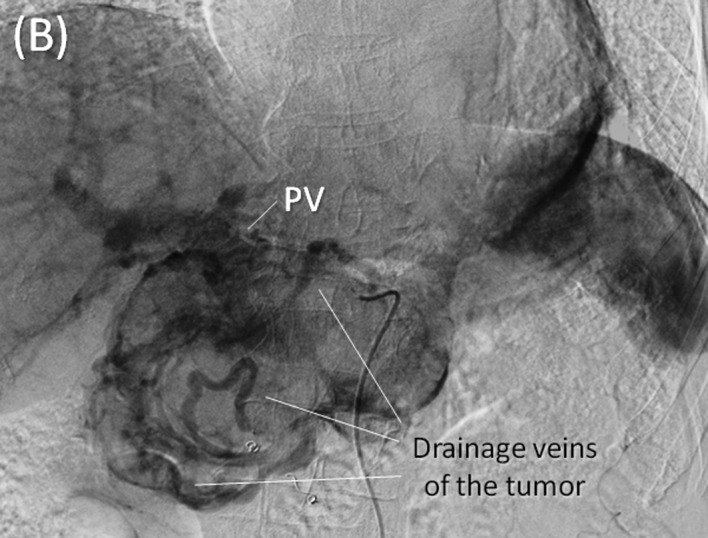
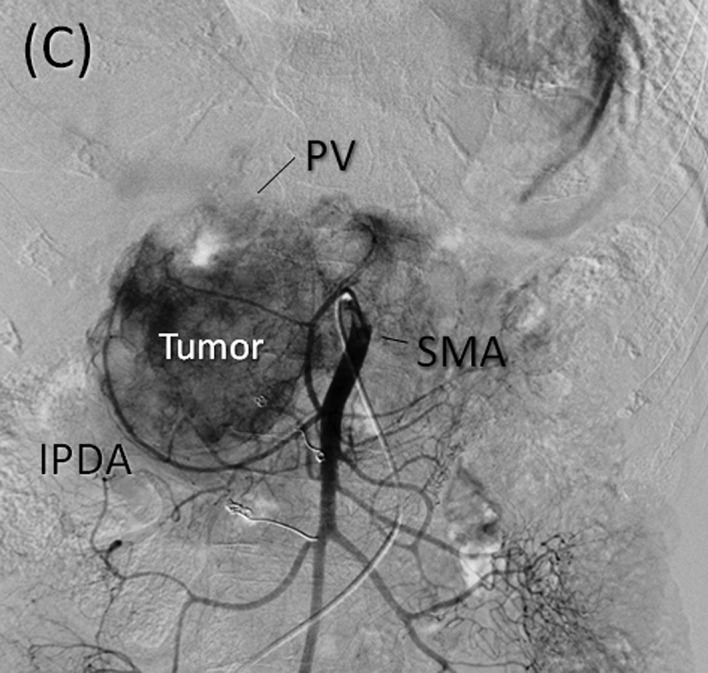
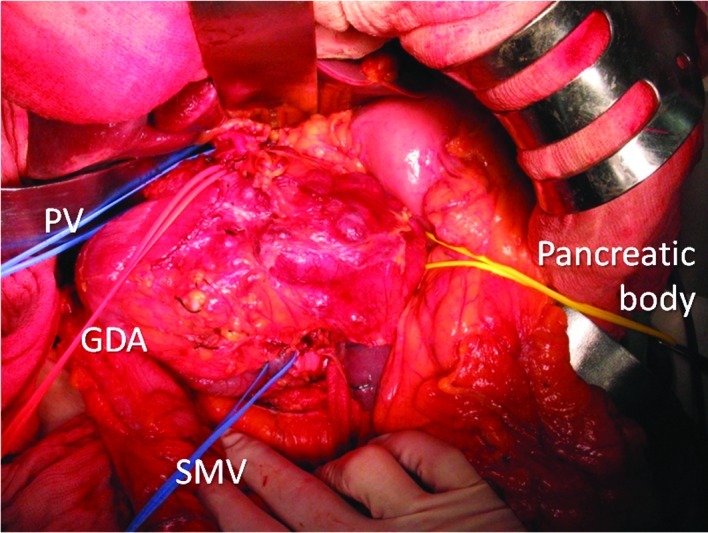
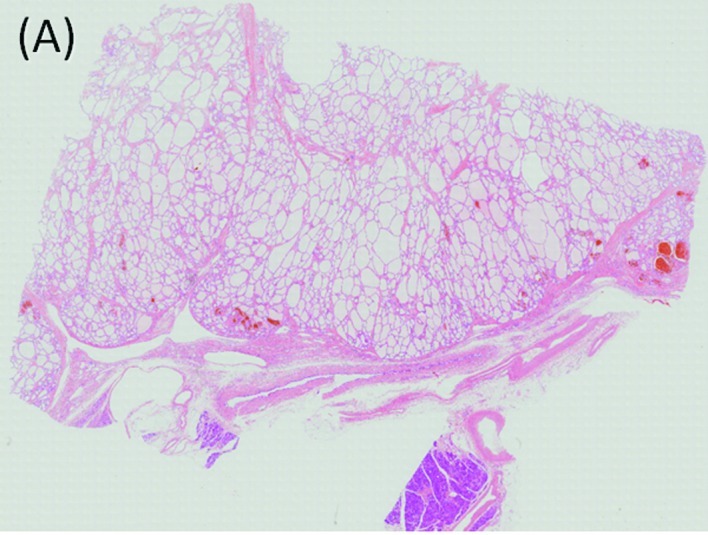
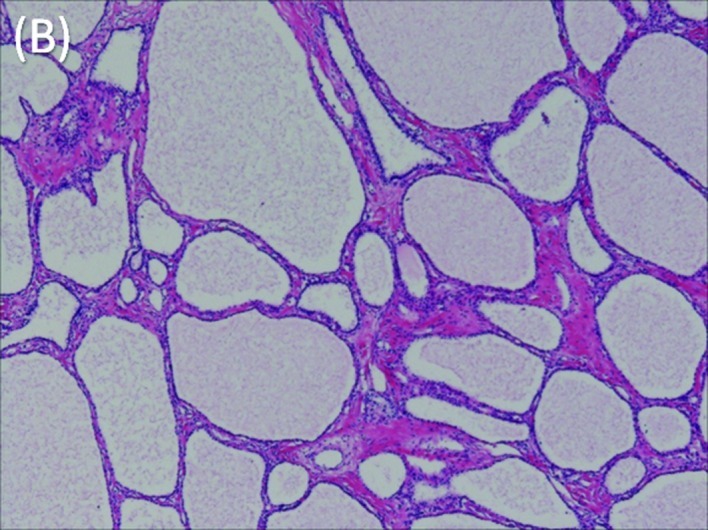
Serous microcystic adenomas are rare and account for 1-2% of all exocrine pancreatic tumors and 25% of all pancreatic cystic neoplasms. Recently, with advances in imaging techniques, these adenomas have been identified at an increasing frequency. A 63-year-old woman visited her doctor in 1999 due to a gastric deformity detected by upper gastrointestinal endoscopy. An abdominal computed tomography scan revealed a cystic lesion measuring 6.0 cm in diameter, resulting in a diagnosis of serous microcystic adenoma of the pancreatic head. During follow-up, the tumor increased steadily in size, measuring 6.0 cm in diameter in 1999 and 13.0 cm in 2008, while remaining asymptomatic throughout this period of time. The risk of malignant transformation appears to be low even over the long-term. However, some cases of malignant transformation to serous cystadenocarcinoma have recently been reported. In this case, assessment of the relationship between the tumor and adjacent vascular structures, such as massive drainage vein development on the surface or tumor flow into the portal and superior mesenteric veins and the celiac and superior mesenteric arteries, was critical for determining tumor resectability. The risk of massive intra-operative hemorrhage was felt to be considerable, given the extent of the veins on the surface of the tumor, as well as the size and location of the primary pancreatic mass. Therefore, preoperative embolization of the tumor-feeding arteries arising from the celiac axis (gastroduodenal, splenic and dorsal pancreatic arteries) was performed. Tumor resection with pancreaticoduodenectomy was performed without a blood transfusion, with an estimated blood loss of 570 ml. The final pathology confirmed the diagnosis of serous microcystic adenoma. The patient is currently alive and disease-free. Preoperative partial embolization of the tumor feeding arteries and intra-operative resection of the right gastric and inferior pancreatoduodenal arteries, allowed the tumor blood supply to be arrested without preoperative tumor necrosis. Subsequently, intraoperative blood loss was reduced. Preoperative partial embolization of the feeding arteries is useful for the resection of hypervascular large tumors of the pancreas.
Figures

Similar articles
-
A case of preoperative embolization for a giant hypervascular pancreatic serous cystic neoplasm in pancreaticoduodenectomy.Surg Case Rep. 2024 Sep 6;10(1):208. doi: 10.1186/s40792-024-02009-2. Surg Case Rep. 2024. PMID: 39237696 Free PMC article.
-
[A safely resected case of hypervascular pancreatic giant tumor after preoperative arterial embolization].Gan To Kagaku Ryoho. 2011 Nov;38(12):2451-3. Gan To Kagaku Ryoho. 2011. PMID: 22202410 Japanese.
-
Giant serous microcystic pancreas adenoma.Rare Tumors. 2012 Oct 10;4(4):e56. doi: 10.4081/rt.2012.e56. Epub 2012 Dec 10. Rare Tumors. 2012. PMID: 23372920 Free PMC article.
-
[Anatomy of the head of the pancreas and various limited resection procedures for intraductal papillary-mucinous tumors of the pancreas].Nihon Geka Gakkai Zasshi. 2003 Jun;104(6):460-70. Nihon Geka Gakkai Zasshi. 2003. PMID: 12854493 Review. Japanese.
-
A giant pancreatic serous microcystic adenoma with 20 years follow-up.Langenbecks Arch Surg. 2007 Mar;392(2):209-13. doi: 10.1007/s00423-006-0146-1. Epub 2007 Jan 19. Langenbecks Arch Surg. 2007. PMID: 17235583 Review.
Cited by
-
A case of preoperative embolization for a giant hypervascular pancreatic serous cystic neoplasm in pancreaticoduodenectomy.Surg Case Rep. 2024 Sep 6;10(1):208. doi: 10.1186/s40792-024-02009-2. Surg Case Rep. 2024. PMID: 39237696 Free PMC article.
-
Intraoperative modulation of arterial blood flow in a hybrid operating room: A report of three cases.Clin Case Rep. 2019 Aug 15;7(10):1839-1843. doi: 10.1002/ccr3.2355. eCollection 2019 Oct. Clin Case Rep. 2019. PMID: 31624594 Free PMC article.
-
Microcystic serous cystadenoma of the pancreas causing biliary obstruction: a case report and review of the literature.J Surg Case Rep. 2024 Mar 8;2024(3):rjae105. doi: 10.1093/jscr/rjae105. eCollection 2024 Mar. J Surg Case Rep. 2024. PMID: 38463732 Free PMC article.
-
Giant Serous Cystadenoma of the Pancreas (⩾10 cm): The Clinical Features and CT Findings.Gastroenterol Res Pract. 2016;2016:8454823. doi: 10.1155/2016/8454823. Epub 2016 Aug 16. Gastroenterol Res Pract. 2016. PMID: 27610132 Free PMC article.
References
-
- Tampi C, Mullerpatan P, Shah R, Jagannath P, Zimmermann A. Microcystic serous cystadenoma of the pancreas: a case report of two cases with one of diffuse presentation. Pancreatology. 2006;6:248–253. - PubMed
-
- Vernadakis S, Kaiser GM, Christodoulou E, Mathe Z, Troullinakis M, Bankfalvi A, Paul A. Enormous serous microcystic adenoma of the pancreas. J Pancreas. 2009;10:332–334. - PubMed
-
- Omeroglu A, Paner GP, Ciesla MC, Harman G. Serous microcystic adenoma of the pancreas. Arch Pathol Lab Med. 2001;125:1613–1614. - PubMed
-
- Schulz HU, Kellner U, Kahl S, Effenberger O, Asperger W, Lippert H, Röcken C. A giant pancreatic serous microcystic adenoma with 20 years follow-up. Langenbecks Arch Surg. 2007;392:209–213. - PubMed
LinkOut - more resources
Full Text Sources