

Virus infection-induced bronchial asthma exacerbation
- PMID: 22966430
- PMCID: PMC3432542
- DOI: 10.1155/2012/834826
Virus infection-induced bronchial asthma exacerbation
Abstract
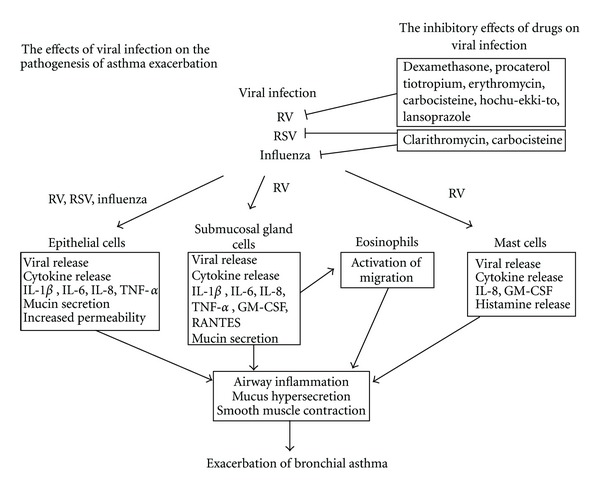
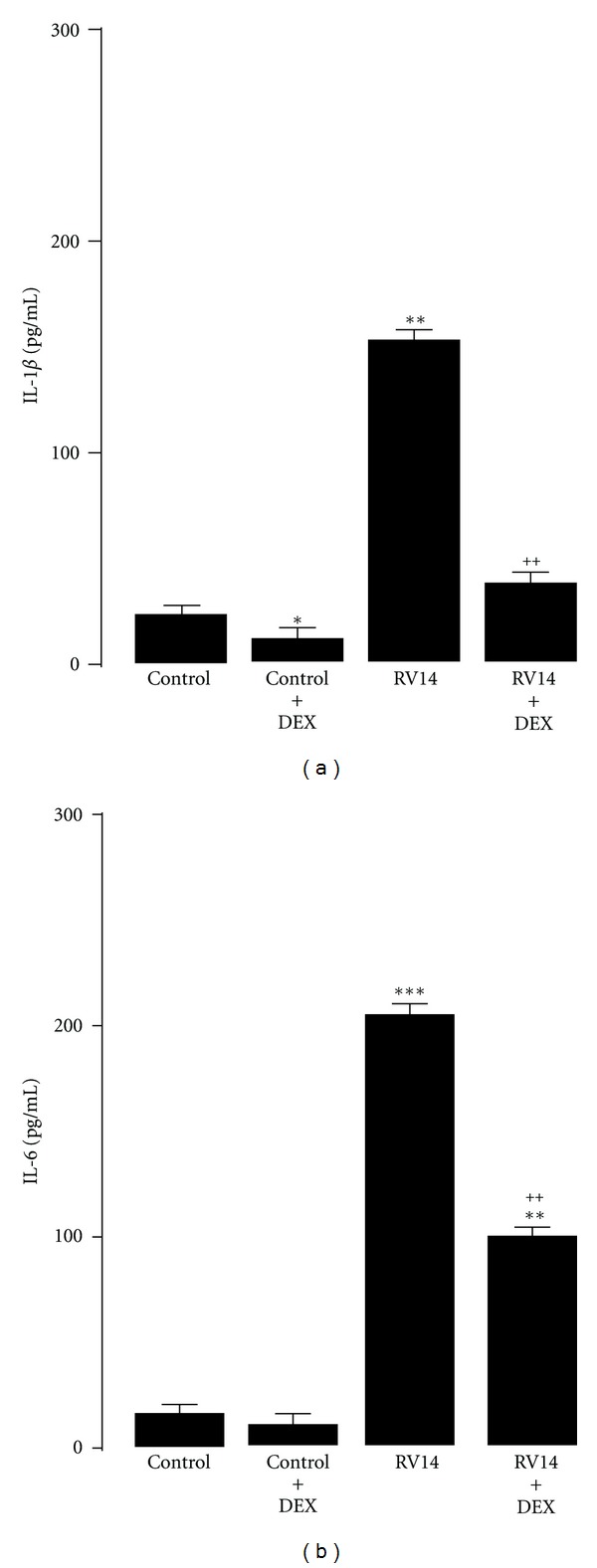
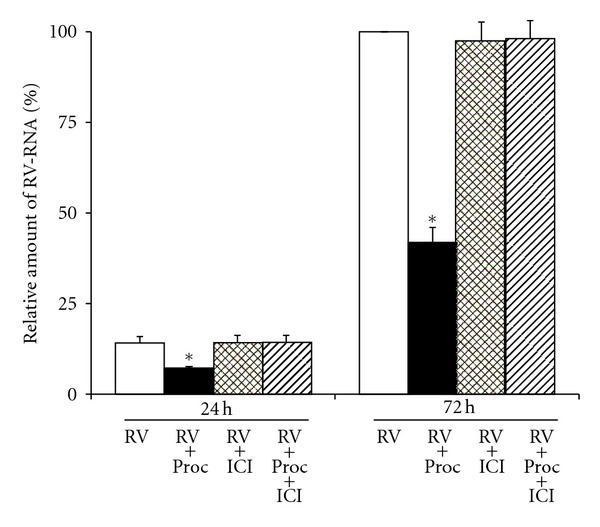
Infection with respiratory viruses, including rhinoviruses, influenza virus, and respiratory syncytial virus, exacerbates asthma, which is associated with processes such as airway inflammation, airway hyperresponsiveness, and mucus hypersecretion. In patients with viral infections and with infection-induced asthma exacerbation, inflammatory mediators and substances, including interleukins (ILs), leukotrienes and histamine, have been identified in the airway secretions, serum, plasma, and urine. Viral infections induce an accumulation of inflammatory cells in the airway mucosa and submucosa, including neutrophils, lymphocytes and eosinophils. Viral infections also enhance the production of inflammatory mediators and substances in airway epithelial cells, mast cells, and other inflammatory cells, such as IL-1, IL-6, IL-8, GM-CSF, RANTES, histamine, and intercellular adhesion molecule-1. Viral infections affect the barrier function of the airway epithelial cells and vascular endothelial cells. Recent reports have demonstrated augmented viral production mediated by an impaired interferon response in the airway epithelial cells of asthma patients. Several drugs used for the treatment of bronchial asthma reduce viral and pro-inflammatory cytokine release from airway epithelial cells infected with viruses. Here, I review the literature on the pathogenesis of the viral infection-induced exacerbation of asthma and on the modulation of viral infection-induced airway inflammation.
Figures
Similar articles
-
Rhinovirus and asthma.Viral Immunol. 2003;16(2):99-109. doi: 10.1089/088282403322017857. Viral Immunol. 2003. PMID: 12828863 Review.
-
Understanding asthma pathophysiology.Allergy Asthma Proc. 2003 Mar-Apr;24(2):79-83. Allergy Asthma Proc. 2003. PMID: 12776439 Review.
-
Involvement and Possible Role of Eosinophils in Asthma Exacerbation.Front Immunol. 2018 Sep 28;9:2220. doi: 10.3389/fimmu.2018.02220. eCollection 2018. Front Immunol. 2018. PMID: 30323811 Free PMC article. Review.
-
Pathogenesis of airway inflammation in bronchial asthma.Auris Nasus Larynx. 2011 Oct;38(5):555-63. doi: 10.1016/j.anl.2011.01.011. Epub 2011 Feb 19. Auris Nasus Larynx. 2011. PMID: 21334836 Review.
-
BuShenYiQi Formula strengthens Th1 response and suppresses Th2-Th17 responses in RSV-induced asthma exacerbated mice.J Ethnopharmacol. 2014 May 28;154(1):131-47. doi: 10.1016/j.jep.2014.03.041. Epub 2014 Apr 3. J Ethnopharmacol. 2014. PMID: 24704667
Cited by
-
Acute effects of viral respiratory tract infections on sputum bacterial density during CF pulmonary exacerbations.J Cyst Fibros. 2015 Jul;14(4):482-9. doi: 10.1016/j.jcf.2014.11.009. Epub 2014 Dec 18. J Cyst Fibros. 2015. PMID: 25544473 Free PMC article.
-
The Effect of Unconventional Cytokine Combinations on NK-Cell Responses to Viral Infection.Front Immunol. 2021 Mar 19;12:645850. doi: 10.3389/fimmu.2021.645850. eCollection 2021. Front Immunol. 2021. PMID: 33815404 Free PMC article. Review.
-
Distal respiratory tract viral infections in young children trigger a marked increase in alveolar mast cells.ERJ Open Res. 2018 Nov 23;4(4):00038-2018. doi: 10.1183/23120541.00038-2018. eCollection 2018 Oct. ERJ Open Res. 2018. PMID: 30480000 Free PMC article.
-
Enhanced airway hyperresponsiveness in asthmatic children and mice with A(H1N1)pdm09 infection.Immun Inflamm Dis. 2021 Jun;9(2):457-465. doi: 10.1002/iid3.406. Epub 2021 Jan 20. Immun Inflamm Dis. 2021. PMID: 33470564 Free PMC article.
-
Screening and functional pathway analysis of genes associated with pediatric allergic asthma using a DNA microarray.Mol Med Rep. 2015 Jun;11(6):4197-203. doi: 10.3892/mmr.2015.3277. Epub 2015 Jan 29. Mol Med Rep. 2015. PMID: 25633562 Free PMC article.
References
-
- Minor TE, Dick EC, Baker JW. Rhinovirus and influenza type A infections as precipitants of asthma. American Review of Respiratory Disease. 1976;113(2):149–153. - PubMed
-
- Gama RE, Horsnell PR, Hughes PJ, et al. Amplification of rhinovirus specific nucleic acids from clinical samples using the polymerase chain reaction. Journal of Medical Virology. 1989;28(2):73–77. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
