

Results of National Colorectal Cancer Screening Program in Croatia (2007-2011)
- PMID: 22969192
- PMCID: PMC3436044
- DOI: 10.3748/wjg.v18.i32.4300
Results of National Colorectal Cancer Screening Program in Croatia (2007-2011)
Abstract
Aim: To study the epidemiologic indicators of uptake and characteristic colonoscopic findings in the Croatian National Colorectal Cancer Screening Program.
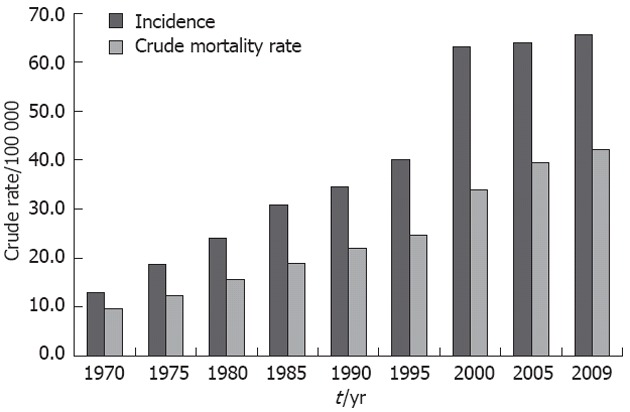
Methods: Colorectal cancer (CRC) was the second leading cause of cancer mortality in men (n = 1063, 49.77/100,000), as well as women (n = 803, 34.89/100,000) in Croatia in 2009. The Croatian National CRC Screening Program was established by the Ministry of Health and Social Welfare, and its implementation started in September, 2007. The coordinators were recruited in each county institute of public health with an obligation to provide fecal occult blood testing (FOBT) to the participants, followed by colonoscopy in all positive cases. The FOBT was performed by hypersensitive guaiac-based Hemognost card test (Biognost, Zagreb). The test and short questionnaire were delivered to the home addresses of all citizens aged 50-74 years consecutively during a 3-year period. Each participant was required to complete the questionnaire and send it together with the stool specimen on three test cards back to the institute for further analysis. About 4% FOBT positive cases are expected in normal risk populations. A descriptive analysis was performed.
Results: A total of 1,056,694 individuals (born between 1933-1945 and 1952-1957) were invited to screening by the end of September 2011. In total, 210,239 (19.9%) persons returned the envelope with a completed questionnaire, and 181,102 of them returned it with a correctly placed stool specimen on FOBT cards. Until now, 12,477 (6.9%), FOBT-positive patients have been found, which is at the upper limit of the expected values in European Guidelines for Quality Assurance in CRC Screening and Diagnosis [European Union (EU) Guidelines]. Colonoscopy was performed in 8541 cases (uptake 66%). Screening has identified CRC in 472 patients (5.5% of colonoscopied, 3.8% of FOBT-positive, and 0.26% of all screened individuals). This is also in the expected range according to EU Guidelines. Polyps were found and removed in 3329 (39% of colonoscopied) patients. The largest number of polyps were found in the left half of the colon: 64% (19%, 37% and 8% in the rectum, sigma, and descendens, respectively). The other 36% were detected in the proximal part (17% in the transverse colon and 19% in ceco-ascending colon). Small polyps in the rectum (5-10 mm in diameter), sigmoid and descending colon were histologically found to be tubular adenomas in 60% of cases, with a low degree of dysplasia, and 40% were classified as hyperplastic. Polyps of this size in the transverse or ceco-ascending colon in almost 20% had a histologically villous component, but still had a low degree of dysplasia. Polyps sized 10-20 mm in diameter were in 43% cases tubulovillous, and among them, 32% had areas with a high degree of dysplasia, especially those polyps in the ceco-ascending or transverse part. The characteristics of the Croatian CRC Screening National Program in the first 3 years were as follows: relatively low percentage of returned FOBT, higher number of FOBT-positive persons but still in the range for population-based programs, and higher number of pathologic findings (polyps and cancers).
Conclusion: These results suggest a need for intervention strategies that include organizational changes and educational activities to improve awareness of CRC screening usefulness and increase participation rates.
Keywords: Colonoscopy; Colorectal cancer screening; Croatian National Colorectal Cancer Screening Program; Fecal occult blood testing; Uptake.
Figures
Similar articles
-
Fecal occult blood test for colorectal cancer screening: an evidence-based analysis.Ont Health Technol Assess Ser. 2009;9(10):1-40. Epub 2009 Sep 1. Ont Health Technol Assess Ser. 2009. PMID: 23074514 Free PMC article.
-
Interval Colorectal Cancer Incidence Among Subjects Undergoing Multiple Rounds of Fecal Immunochemical Testing.Gastroenterology. 2017 Aug;153(2):439-447.e2. doi: 10.1053/j.gastro.2017.05.004. Epub 2017 May 5. Gastroenterology. 2017. PMID: 28483499
-
Early Detection of Colorectal Cancer: a Multi-Center Pre-Clinical Case Cohort Study for Validation of a Combined DNA Stool Test.Clin Lab. 2018 Oct 1;64(10):1719-1730. doi: 10.7754/Clin.Lab.2018.180521. Clin Lab. 2018. PMID: 30336540
-
[Chemical or immunological tests for the detection of fecal occult blood in colorectal cancer screening?].Gastroenterol Hepatol. 2009 Oct;32(8):565-76. doi: 10.1016/j.gastrohep.2009.01.179. Epub 2009 Jul 3. Gastroenterol Hepatol. 2009. PMID: 19577340 Review. Spanish.
-
Colorectal cancer screening: 20 years of development and recent progress.World J Gastroenterol. 2014 Apr 14;20(14):3825-34. doi: 10.3748/wjg.v20.i14.3825. World J Gastroenterol. 2014. PMID: 24744575 Free PMC article. Review.
Cited by
-
Incidence and mortality trends of gastric and colorectal cancers in Croatia, 1988-2008.Croat Med J. 2012 Apr;53(2):124-34. doi: 10.3325/cmj.2012.53.124. Croat Med J. 2012. PMID: 22522990 Free PMC article.
-
Microbial markers in colorectal cancer detection and/or prognosis.World J Gastroenterol. 2018 Jun 14;24(22):2327-2347. doi: 10.3748/wjg.v24.i22.2327. World J Gastroenterol. 2018. PMID: 29904241 Free PMC article. Review.
-
Diagnosis and natural history of preclinical and early inflammatory bowel disease.Ann Gastroenterol. 2020 Sep-Oct;33(5):443-452. doi: 10.20524/aog.2020.0508. Epub 2020 Jun 22. Ann Gastroenterol. 2020. PMID: 32879589 Free PMC article. Review.
-
Recent Advances and Potential Multi-Omics Approaches in the Early Phases of Inflammatory Bowel Disease.J Clin Med. 2023 May 11;12(10):3418. doi: 10.3390/jcm12103418. J Clin Med. 2023. PMID: 37240524 Free PMC article. Review.
-
Organised colorectal cancer screening in Lampang Province, Thailand: preliminary results from a pilot implementation programme.BMJ Open. 2014 Jan 15;4(1):e003671. doi: 10.1136/bmjopen-2013-003671. BMJ Open. 2014. PMID: 24435889 Free PMC article.
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–2917. - PubMed
-
- Levin B, Lieberman DA, McFarland B, Smith RA, Brooks D, Andrews KS, Dash C, Giardiello FM, Glick S, Levin TR, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin. 2008;58:130–160. - PubMed
-
- Znaor A. Cancer Incidence in Croatia 2008. Zagreb: Croatian National Institute of Public Health; 2009.
-
- Čorić T, Mihel S, Miler A, Ivičević Uhernik A, Pristaš I, Petruša B. Umrle osobe u Hrvatskoj u 2010. godini, Hrvatski zavod za javno zdravstvo, zagreb srpanj 2011. Available from: http: //www.hzjz.hr/publikacije/umrli_2010.pdf.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
