

Evaluation of magnifying colonoscopy in the diagnosis of serrated polyps
- PMID: 22969193
- PMCID: PMC3436045
- DOI: 10.3748/wjg.v18.i32.4308
Evaluation of magnifying colonoscopy in the diagnosis of serrated polyps
Abstract
Aim: To elucidate the colonoscopic features of serrated lesions of the colorectum using magnifying colonoscopy.
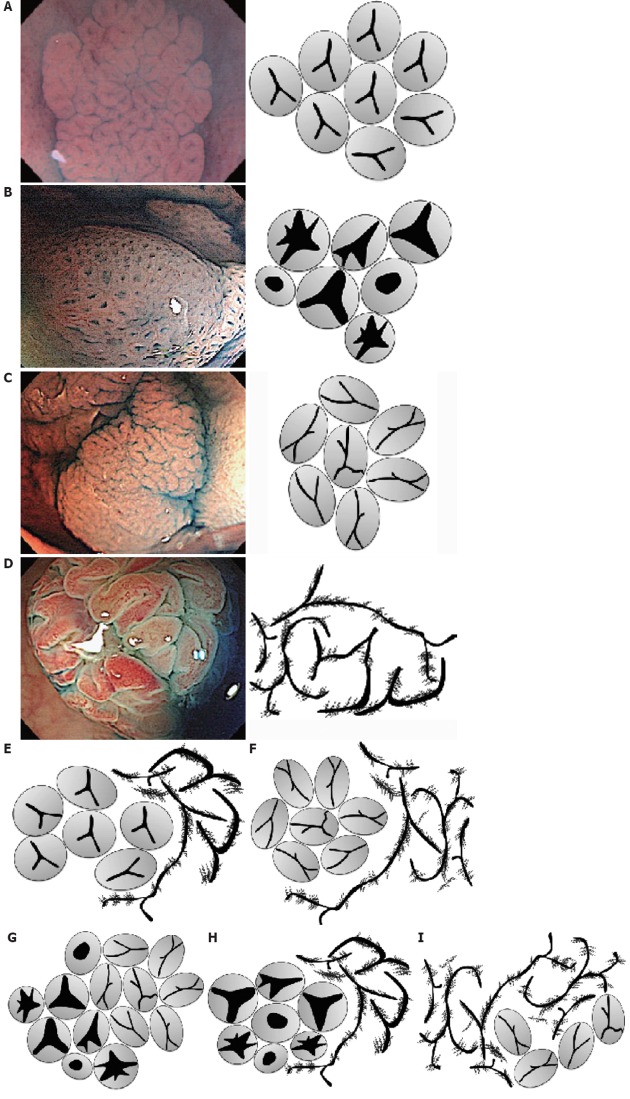
Methods: Broad division of serrated lesions of the colorectum into hyperplastic polyps (HPs), traditional serrated adenomas (TSAs), and sessile serrated adenomas/polyps (SSA/Ps) has been proposed on the basis of recent molecular biological studies. However, few reports have examined the colonoscopic features of these divisions, including magnified colonoscopic findings. This study examined 118 lesions excised in our hospital as suspected serrated lesions after magnified observation between January 2008 and September 2011. Patient characteristics (sex, age), conventional colonoscopic findings (location, size, morphology, color, mucin) and magnified colonoscopic findings (pit pattern diagnosis) were interpreted by five colonoscopists with experience in over 1000 colonoscopies, and were compared with histopathological diagnoses. The pit patterns were categorized according to Kudo's classification, but a more detailed investigation was also performed using the subclassification [type II-Open (type II-O), type II-Long (type II-L), or type IV-Serrated (type IV-S)] proposed by Kimura T and Yamano H.
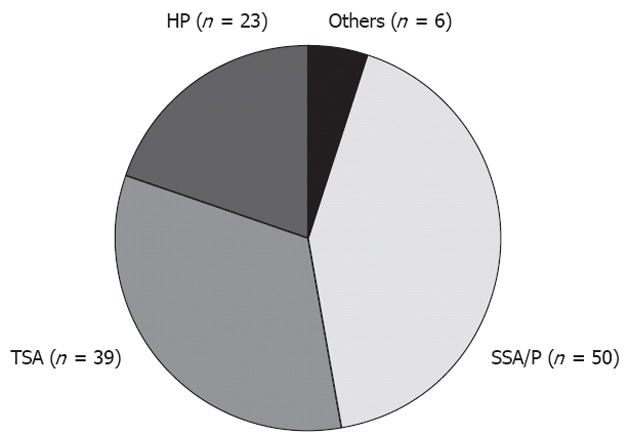
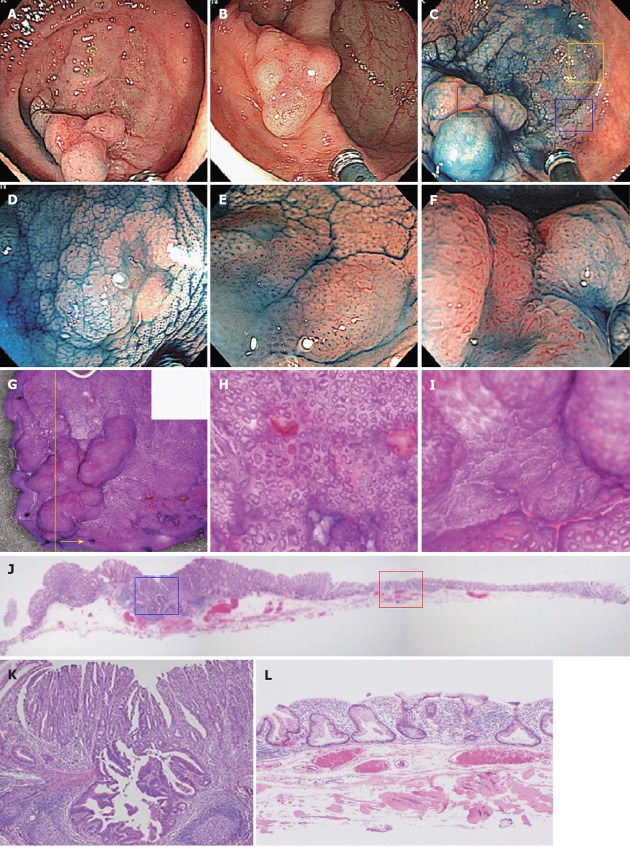
Results: Lesions comprised 23 HPs (23/118: 19.5%), 39 TSAs (39/118: 33.1%: with cancer in one case), 50 SSA/Ps (50/118: 42.4%: complicated with cancer in three cases), and six others (6/118: 5.1%). We excluded six others, including three regular adenomas, one hamartoma, one inflammatory polyp, and one juvenile polyp for further analysis. Conventional colonoscopy showed that SSA/Ps were characterized as larger in diameter than TSAs and HPs (SSA/P vs HP, 13.62 ± 8.62 mm vs 7.74 ± 3.24 mm, P < 0.001; SSA/Ps vs TSA, 13.62 ± 8.62 mm vs 9.89 ± 5.73 mm, P < 0.01); common in the right side of the colon [HPs, 30.4% (7/23): TSAs, 20.5% (8/39): SSA/P, 84.0% (42/50), P < 0.001]; flat-elevated lesion [HPs, 30.4% (7/23): TSAs, 5.1% (2/39): SSA/Ps, 90.0% (45/50), P < 0.001]; normal-colored or pale imucosa [HPs, 34.8% (8/23): TSAs, 10.3% (4/39): SSA/Ps, 80% (40/50), P < 0.001]; and with large amounts of mucin [HPs, 21.7% (5/23): TSAs, 17.9% (7/39): SSA/Ps, 72.0% (36/50), P < 0.001]. In magnified colonoscopic findings, 17 lesions showed either type II pit pattern alone or partial type II pit pattern as the basic architecture, with 14 HPs (14/17, 70.0%) and 3 SSA/Ps. Magnified colonoscopy showed the type II-O pit pattern as characteristic of SSA/Ps [sensitivity 83.7% (41/49), specificity 85.7% (54/63)]. Cancer was also present in three lesions, in all of which a type VI pit pattern was also present within the same lesion. There were four HPs and four TSAs each. The type IV-S pit pattern was characteristic of TSAs [sensitivity 96.7% (30/31), specificity 89.9% (72/81)]. Cancer was present in one lesion, in which a type VI pit pattern was also present within the same lesion. In our study, serrated lesions of the colorectum also possessed the features described in previous reports of conventional colonoscopic findings. The pit pattern diagnosis using magnifying colonoscopy, particularly magnified colonoscopic findings using subclassifications of surface architecture, reflected the pathological characteristics of SSA/Ps and TSAs, and will be useful for colonoscopic diagnosis.
Conclusion: We suggest that this system could be a good diagnostic tool for SSA/Ps using magnifying colonoscopy.
Keywords: Conventional colonoscopy; Hyperplastic polyps; Magnifying colonoscopy; Pit patterns; Serrated adenoma; Serrated lesions; Sessile serrated adenoma/polyp; Traditional serrated adenomas.
Figures
References
-
- Vogelstein B, Fearon ER, Hamilton SR, Kern SE, Preisinger AC, Leppert M, Nakamura Y, White R, Smits AM, Bos JL. Genetic alterations during colorectal-tumor development. N Engl J Med. 1988;319:525–532. - PubMed
-
- Hawkins NJ, Bariol C, Ward RL. The serrated neoplasia pathway. Pathology. 2002;34:548–555. - PubMed
-
- Jass JR, Young J, Leggett BA. Hyperplastic polyps and DNA microsatellite unstable cancers of the colorectum. Histopathology. 2000;37:295–301. - PubMed
-
- Jass JR. Serrated adenoma and colorectal cancer. J Pathol. 1999;187:499–502. - PubMed
-
- Leggett B, Whitehall V. Role of the serrated pathway in colorectal cancer pathogenesis. Gastroenterology. 2010;138:2088–2100. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
