

Adalimumab in prevention of postoperative recurrence of Crohn's disease in high-risk patients
- PMID: 22969204
- PMCID: PMC3436056
- DOI: 10.3748/wjg.v18.i32.4391
Adalimumab in prevention of postoperative recurrence of Crohn's disease in high-risk patients
Abstract
Aim: To evaluate the effectiveness of adalimumab in preventing recurrence after intestinal resection for Crohn's disease in high-risk patients.
Methods: A multicenter, prospective, observational study was conducted from June 2009 until June 2010. We consecutively included high-risk Crohn's disease patients who had undergone an ileal/ileocolonic resection. High-risk patients were defined as two or more criteria: smokers, penetrating pattern, one or more previous surgical resections or prior extensive resection. Subcutaneous adalimumab was administered 2 wk (± 5 d) after surgery at a dose of 40 mg eow, with an initial induction dose of 160/80 mg at weeks 0 and 2. Demographic data, previous and concomitant treatments (antibiotics, 5-aminosalicylates, corticosteroids, immunomodulators or biologic therapies), smoking status at the time of diagnosis and after the index operation and number of previous resections (type and reason for surgery) were all recorded. Biological status was assessed with C-reactive protein, erythrocyte sedimentation rate and fecal calprotectin. One year (± 3 mo) after surgery, an ileocolonoscopy and/or magnetic resonance enterography was performed. Endoscopic recurrence was defined as Rutgeerts score ≥ i2. Morphological recurrence was based on magnetic resonance (MR) score ≥ MR1.
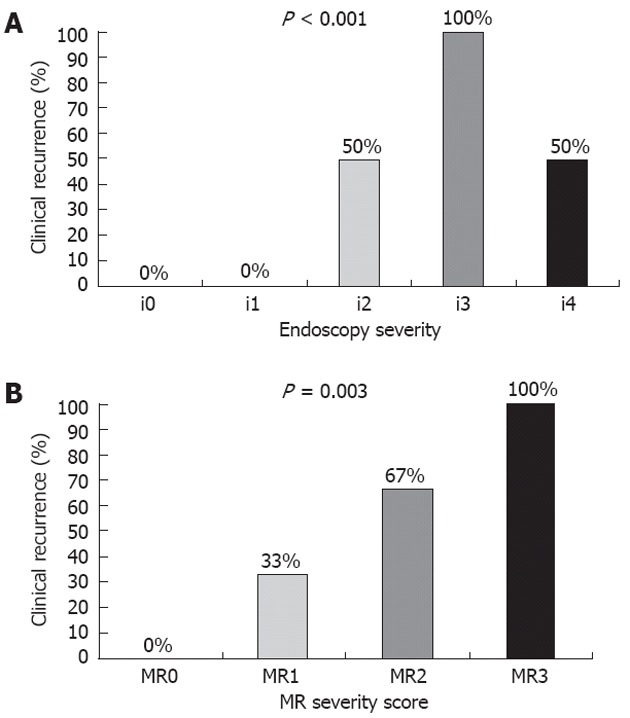
Results: Twenty-nine patients (55.2% males, 48.3% smokers at diagnosis and 13.8% after the index operation), mean age 42.3 years and mean duration of the disease 13.8 years were included in the study. A mean of 1.76 (range: 1-4) resections previous to adalimumab administration and in 37.9% was considered extensive resection. 51.7% had previously received infliximab. Immunomodulators were given concomitantly to 17.2% of patients. Four of the 29 (13.7%) developed clinical recurrence, 6/29 (20.7%) endoscopic recurrence and 7/19 (36.8%) morphological recurrence after 1-year. All patients with clinical recurrence showed endoscopic and morphological recurrence. A high degree of concordance was found between clinical-endoscopic recurrence (κ = 0.76, P < 0.001) and clinical-morphological recurrence (κ = 0.63, P = 0.003). Correlation between endoscopic and radiological findings was good (comparing the 5-point Rutgeerts score with the 4-point MR score, a score of i4 was classified as MR3, i3 as MR2, and i2-i1 as MR1) (P < 0.001, r(s) = 0.825). During follow-up, five (17.2%) patients needed adalimumab dose intensification (40 mg/wk); Mean time to intensification after the introduction of adalimumab treatment was 8 mo (range: 5 to 11 mo). In three cases (10.3%), a biological change was needed due to a worsening of the disease after the dose intensification to 40 mg/wk. One patient suffered an adverse event.
Conclusion: Adalimumab seems to be effective and safe in preventing postoperative recurrence in a selected group of patients who had undergone an intestinal resection for their CD.
Keywords: Adalimumab; Crohn’s disease; Postoperative recurrence; Prevention; Tumor necrosis factor alpha agents.
Figures
References
-
- Loftus EV, Schoenfeld P, Sandborn WJ. The epidemiology and natural history of Crohn’s disease in population-based patient cohorts from North America: a systematic review. Aliment Pharmacol Ther. 2002;16:51–60. - PubMed
-
- Jess T, Riis L, Vind I, Winther KV, Borg S, Binder V, Langholz E, Thomsen OØ, Munkholm P. Changes in clinical characteristics, course, and prognosis of inflammatory bowel disease during the last 5 decades: a population-based study from Copenhagen, Denmark. Inflamm Bowel Dis. 2007;13:481–489. - PubMed
-
- Rutgeerts P, Geboes K, Vantrappen G, Beyls J, Kerremans R, Hiele M. Predictability of the postoperative course of Crohn’s disease. Gastroenterology. 1990;99:956–963. - PubMed
-
- Sailer J, Peloschek P, Reinisch W, Vogelsang H, Turetschek K, Schima W. Anastomotic recurrence of Crohn’s disease after ileocolic resection: comparison of MR enteroclysis with endoscopy. Eur Radiol. 2008;18:2512–2521. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
