

Resting state networks and consciousness: alterations of multiple resting state network connectivity in physiological, pharmacological, and pathological consciousness States
- PMID: 22969735
- PMCID: PMC3427917
- DOI: 10.3389/fpsyg.2012.00295
Resting state networks and consciousness: alterations of multiple resting state network connectivity in physiological, pharmacological, and pathological consciousness States
Abstract
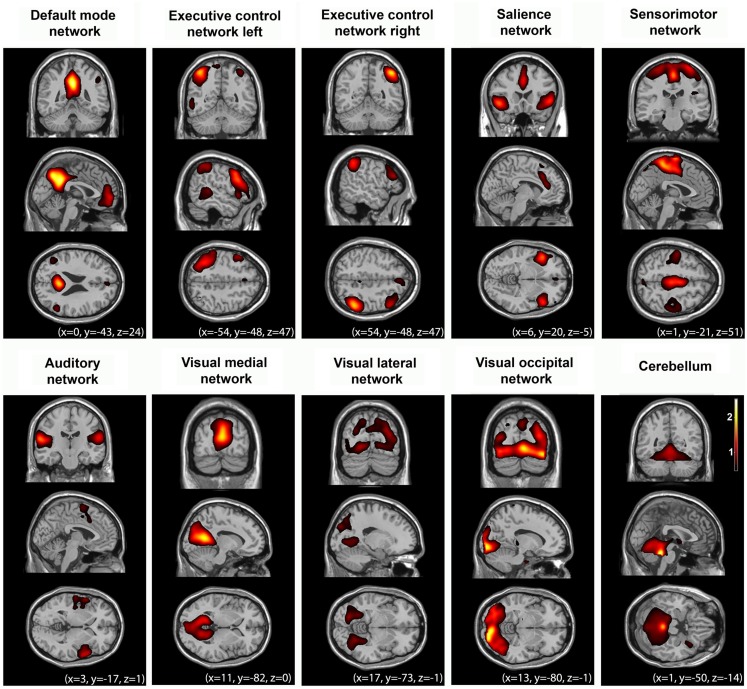
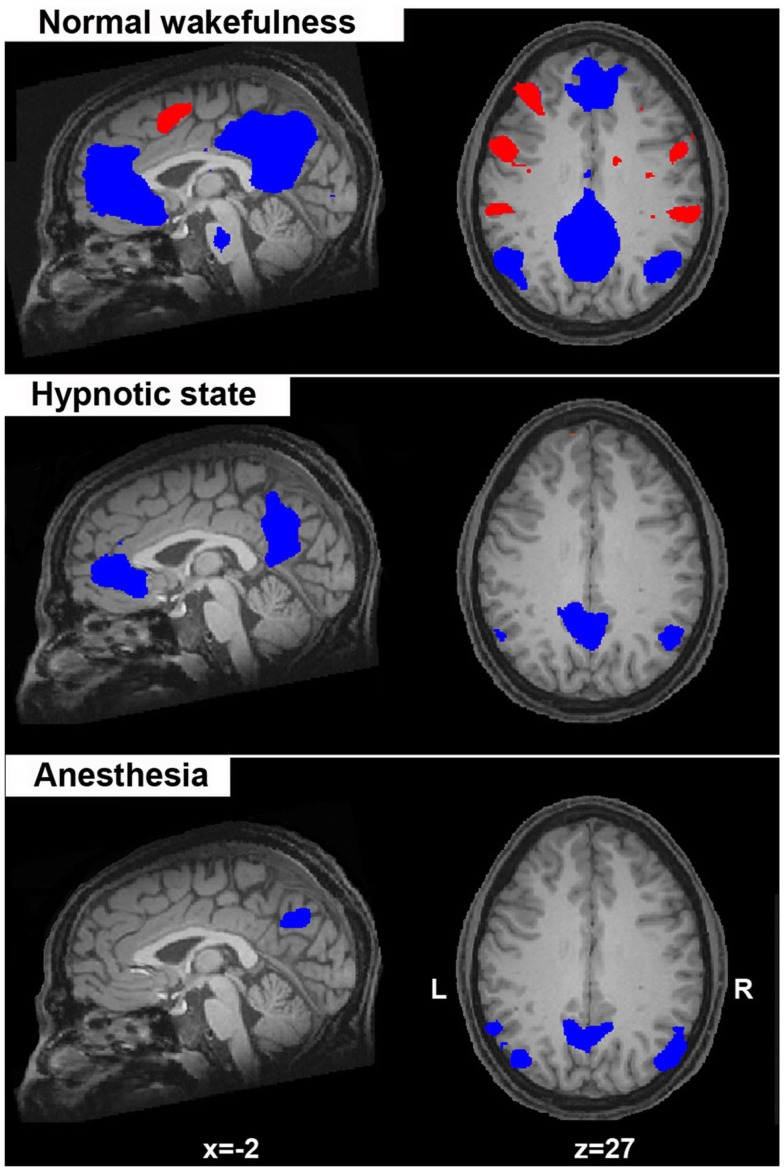
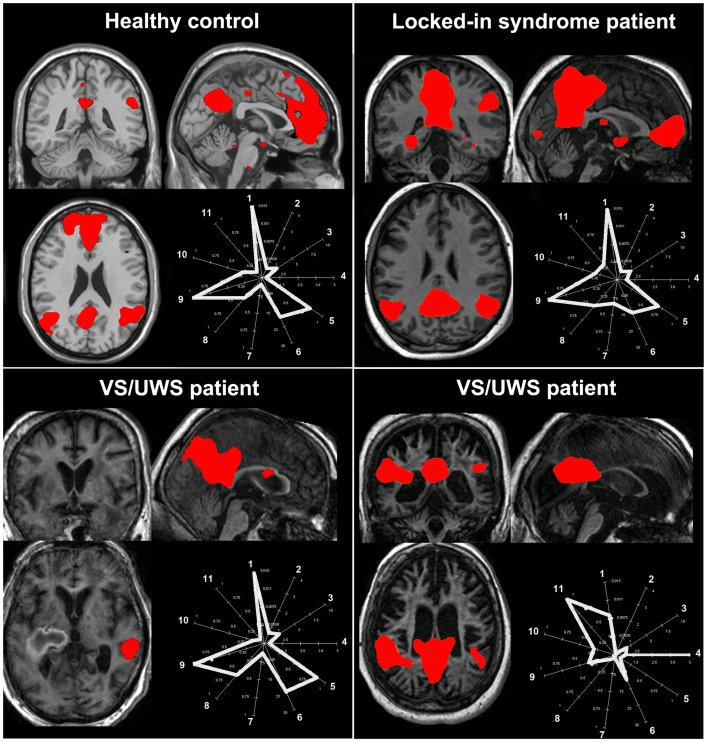
In order to better understand the functional contribution of resting state activity to conscious cognition, we aimed to review increases and decreases in functional magnetic resonance imaging (fMRI) functional connectivity under physiological (sleep), pharmacological (anesthesia), and pathological altered states of consciousness, such as brain death, coma, vegetative state/unresponsive wakefulness syndrome, and minimally conscious state. The reviewed resting state networks were the DMN, left and right executive control, salience, sensorimotor, auditory, and visual networks. We highlight some methodological issues concerning resting state analyses in severely injured brains mainly in terms of hypothesis-driven seed-based correlation analysis and data-driven independent components analysis approaches. Finally, we attempt to contextualize our discussion within theoretical frameworks of conscious processes. We think that this "lesion" approach allows us to better determine the necessary conditions under which normal conscious cognition takes place. At the clinical level, we acknowledge the technical merits of the resting state paradigm. Indeed, fast and easy acquisitions are preferable to activation paradigms in clinical populations. Finally, we emphasize the need to validate the diagnostic and prognostic value of fMRI resting state measurements in non-communicating brain damaged patients.
Keywords: anesthesia; coma; consciousness; default mode network; hypnosis; resting state networks; sleep.
Figures
References
-
- Allen E. A., Erhardt E. B., Damaraju E., Gruner W., Segall J. M., Silva R. F., Havlicek M., Rachakonda S., Fries J., Kalyanam R., Michael A. M., Caprihan A., Turner J. A., Eichele T., Adelsheim S., Bryan A. D., Bustillo J., Clark V. P., Feldstein Ewing S. W., Filbey F., Ford C. C., Hutchison K., Jung R. E., Kiehl K. A., Kodituwakku P., Komesu Y. M., Mayer A. R., Pearlson G. D., Phillips J. P., Sadek J. R., Stevens M., Teuscher U., Thoma R. J., Calhoun V. D. (2011). A baseline for the multivariate comparison of resting-state networks. Front. Syst. Neurosci. 5:2. 10.3389/fnsys.2011.00002 - DOI - PMC - PubMed
-
- American Society of Anesthesiologists Task Force on Intraoperative Awareness (2006). Practice advisory for intraoperative awareness and brain function monitoring a report by the American society of anesthesiologists task force on intraoperative awareness. Anesthesiology 104, 847–864 10.1097/00000542-200604000-00031 - DOI - PubMed
-
- Bardin J. C., Fins J. J., Katz D. I., Hersh J., Heier L. A., Tabelow K., Dyke J. P., Ballon D. J., Schiff N. D., Voss H. U. (2011). Dissociations between behavioural and functional magnetic resonance imaging-based evaluations of cognitive function after brain injury. Brain 134, 769–782 10.1093/brain/awr005 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources