

A Single-Centre Study of Acute Cardiorenal Syndrome: Incidence, Risk Factors and Consequences
- PMID: 22969772
- PMCID: PMC3433012
- DOI: 10.1159/000337714
A Single-Centre Study of Acute Cardiorenal Syndrome: Incidence, Risk Factors and Consequences
Abstract
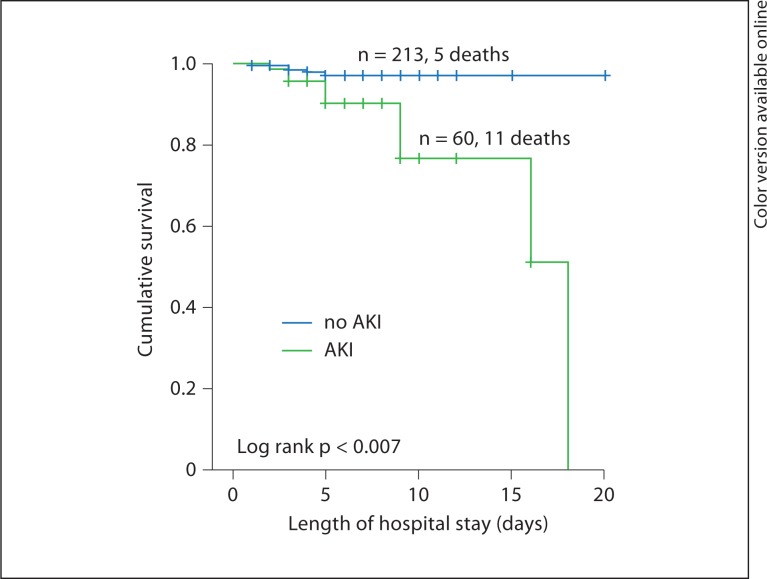
OBJECTIVE: Cardiac and kidney diseases are common, and the impact of acute kidney injury (AKI) on patient outcome is well known. We aimed to investigate the incidence of acute cardiorenal syndrome (CRS) and the risk factors and outcomes associated with the disease. METHODS: We conducted a retrospective cohort study comprising 289 patients with acute coronary syndrome (ACS) and acute decompensated heart failure (ADHF), examining the incidence of AKI defined according to the Acute Kidney Injury Network (AKIN) classification, the factors contributing to AKI, and the impact of AKI on in-hospital mortality and hospital re-admission. RESULTS: Of 71 patients with AKI, 36 (50.7%) had ACS and 35 (49%) had ADHF. Overall in-hospital mortality was 5.5% (n = 16). Multivariate logistic regression identified the following independent predictors of AKI in male patients with ACS: previous myocardial infarction at age >65 years (OR 5.967, 95% CI 1.16-30.47, p = 0.03), chronic kidney disease (OR 3.72, 95% CI 1.31-16.61, p = 0.01), and decreased hemoglobin levels (OR 0.684, 95% CI 0.53-0.88, p = 0.03). No variable was identified as an independent risk factor in ADHF patients. Kaplan-Meier survival curves indicated that patients with ACS plus AKI had significantly higher in-hospital mortality (log rank = 0.007). CONCLUSION: Acute CRS (type 1 CRS) is more frequent in patients with ADHF and can be considered multifactorial. Although CRS is less frequent in ACS patients, it is associated with longer hospital stay and with higher in-hospital mortality. The heart-kidney interaction should be managed collaboratively between cardiologists and nephrologists to increase our knowledge and enhance clinical approaches.
Figures
References
-
- Efendigil MC, Harley A, Deegan T, McKendrick CS. Changes in glomerular filtration rate following myocardial infarction. Cardiovasc Res. 1975;9:741–744. - PubMed
-
- Smith GL, Vaccarino V, Kosiborod M, Lichtman JH, Cheng S, Watnick SG, et al. Worsening renal function: what is a clinically meaningful change in creatinine during hospitalization with heart failure? J Card Fail. 2003;9:13–25. - PubMed
-
- Lourenco C, Teixeira R, António N, Monteiro S, Baptista R, Jorge E, et al. Impact of renal function on mortality and incidence of major adverse cardiovascular events following acute coronary syndromes. Rev Port Cardiol. 2010;29:1331–1352. - PubMed
-
- Ronco C, Ronco F. Cardio-renal syndromes: a systematic approach for consensus definition and classification. Heart Fail Rev. 2011 E-pub ahead of print. - PubMed
LinkOut - more resources
Full Text Sources