

Mapping the aetiology of non-malarial febrile illness in Southeast Asia through a systematic review--terra incognita impairing treatment policies
- PMID: 22970193
- PMCID: PMC3435412
- DOI: 10.1371/journal.pone.0044269
Mapping the aetiology of non-malarial febrile illness in Southeast Asia through a systematic review--terra incognita impairing treatment policies
Abstract
Background: An increasing use of point of care diagnostic tests that exclude malaria, coupled with a declining malaria burden in many endemic countries, is highlighting the lack of ability of many health systems to manage other causes of febrile disease. A lack of knowledge of distribution of these pathogens, and a lack of screening and point-of-care diagnostics to identify them, prevents effective management of these generally treatable contributors to disease burden. While prospective data collection is vital, an untapped body of knowledge already exists in the published health literature.
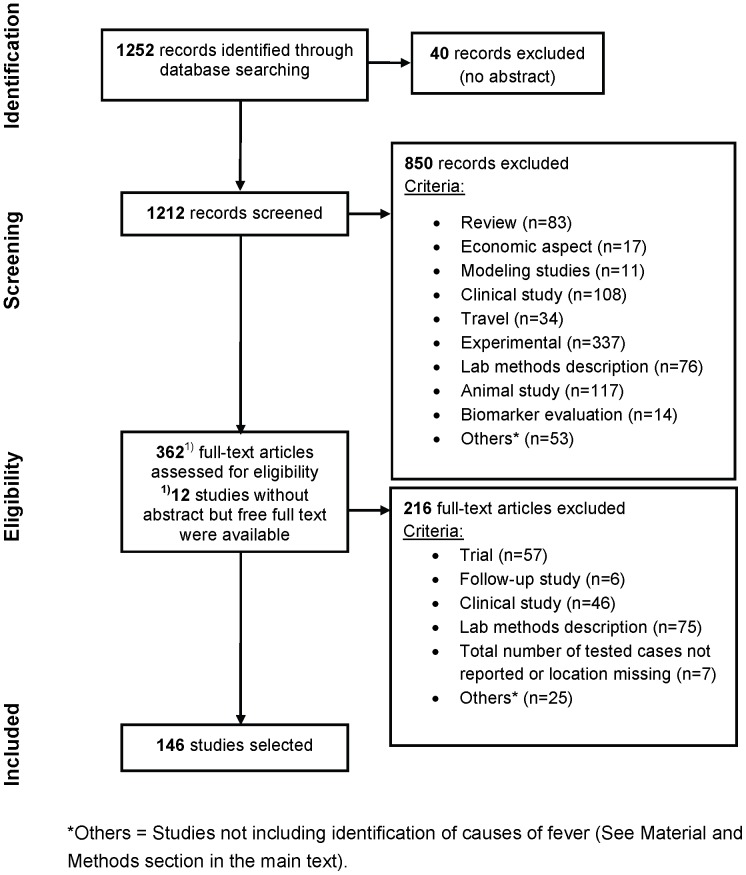
Methods: Focusing on the Mekong region of Southeast Asia, published data from 1986 to 2011 was screened to for frequency of isolation of pathogens implicated in aetiology of non-malarial febrile illness. Eligibility criteria included English-language peer-reviewed studies recording major pathogens for which specific management is likely to be warranted. Of 1,252 identified papers, 146 met inclusion criteria and were analyzed and data mapped.
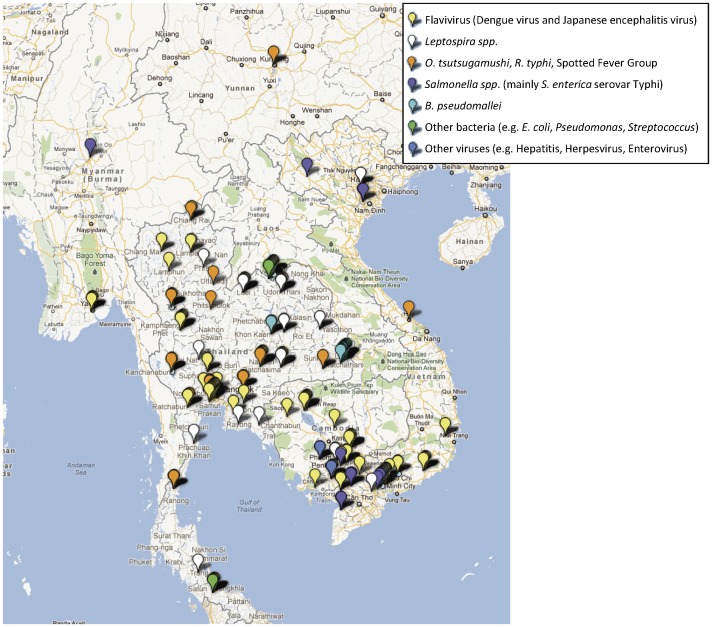
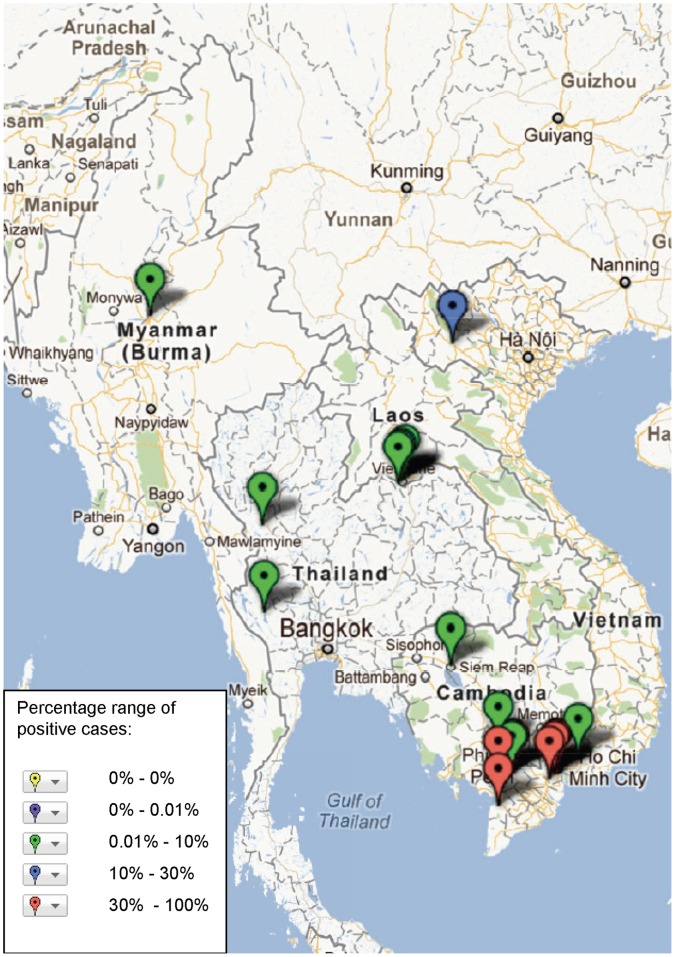
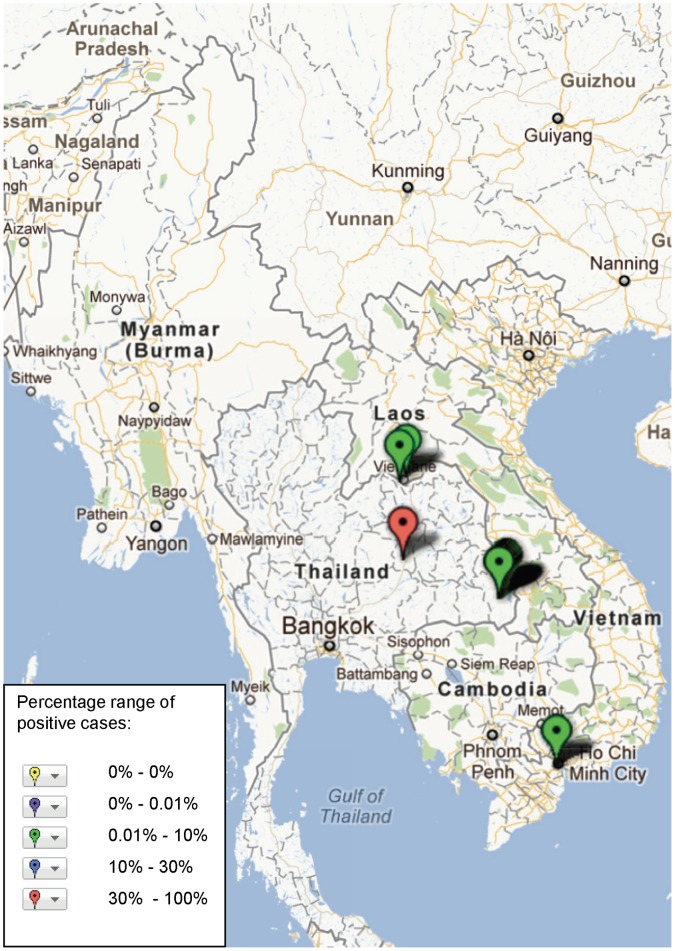
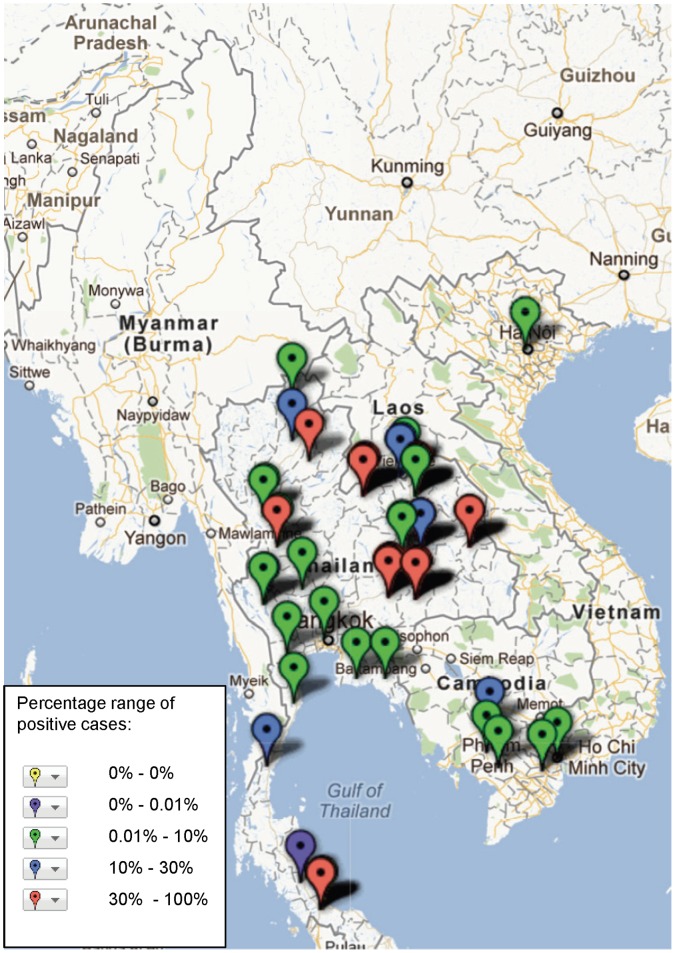
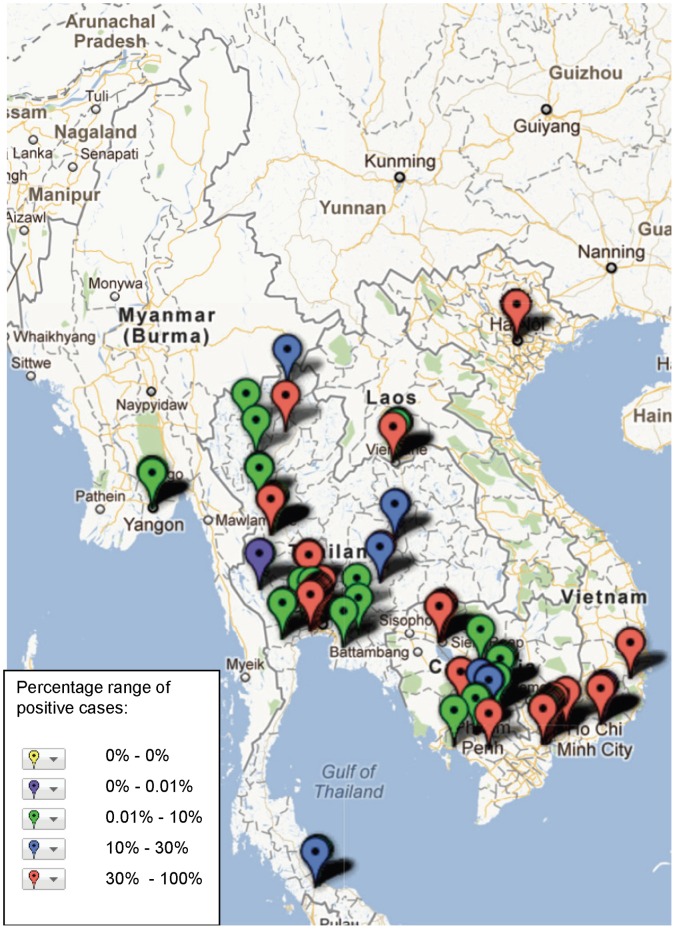
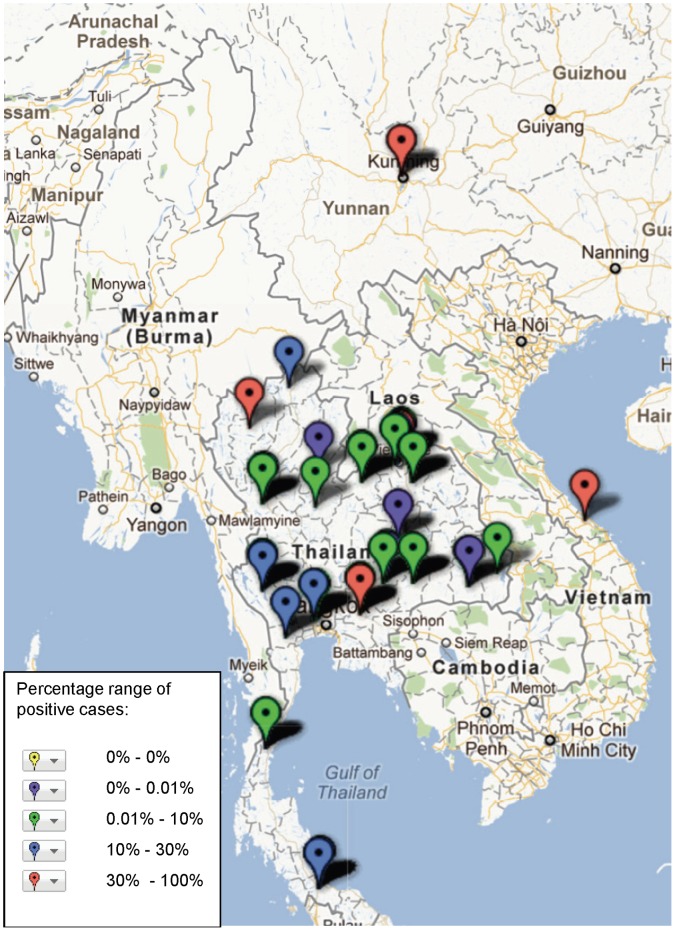
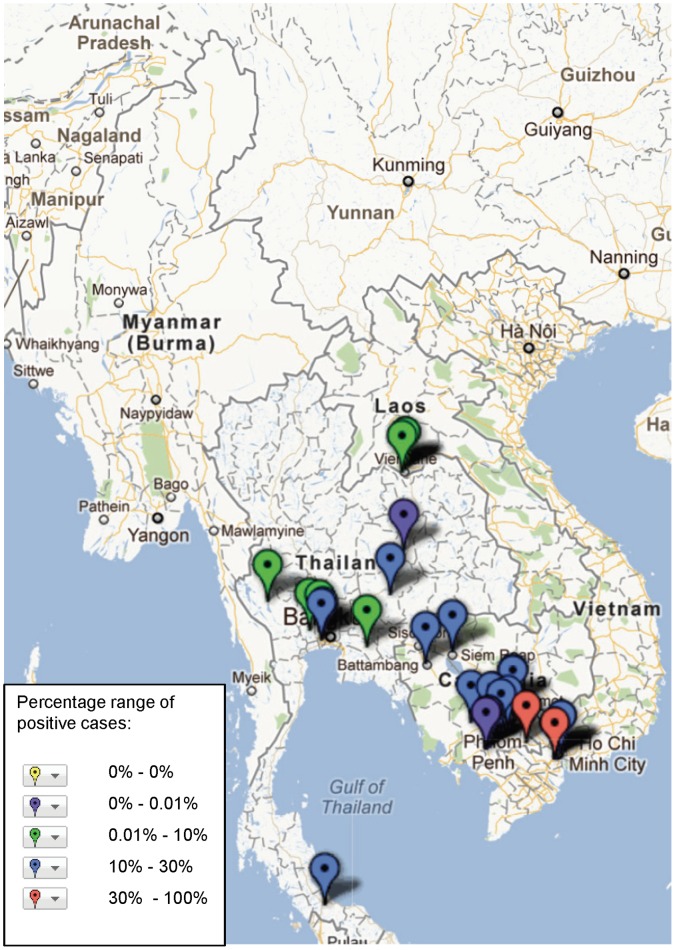
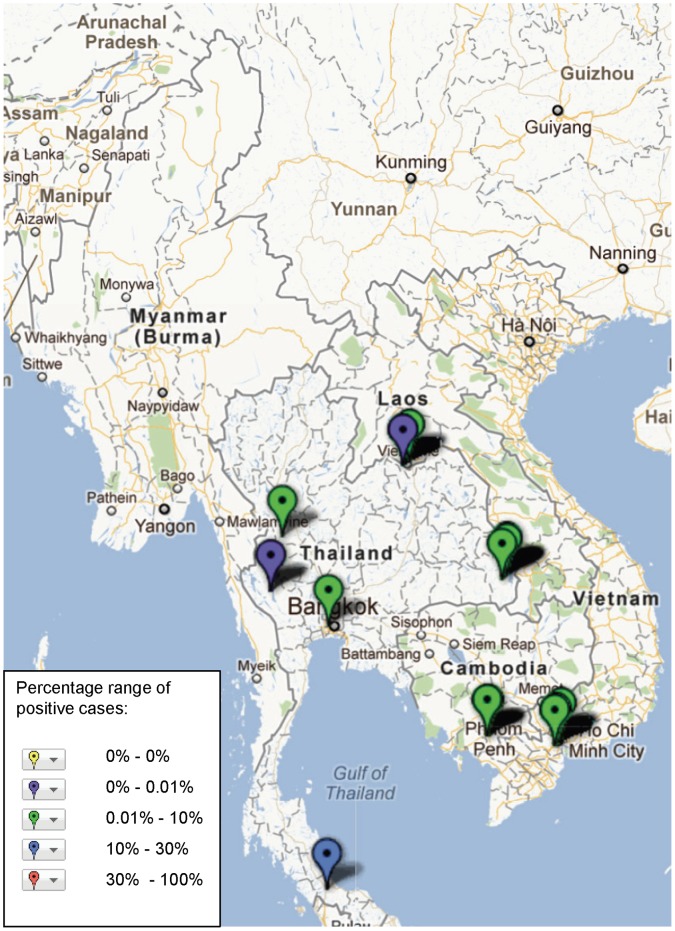
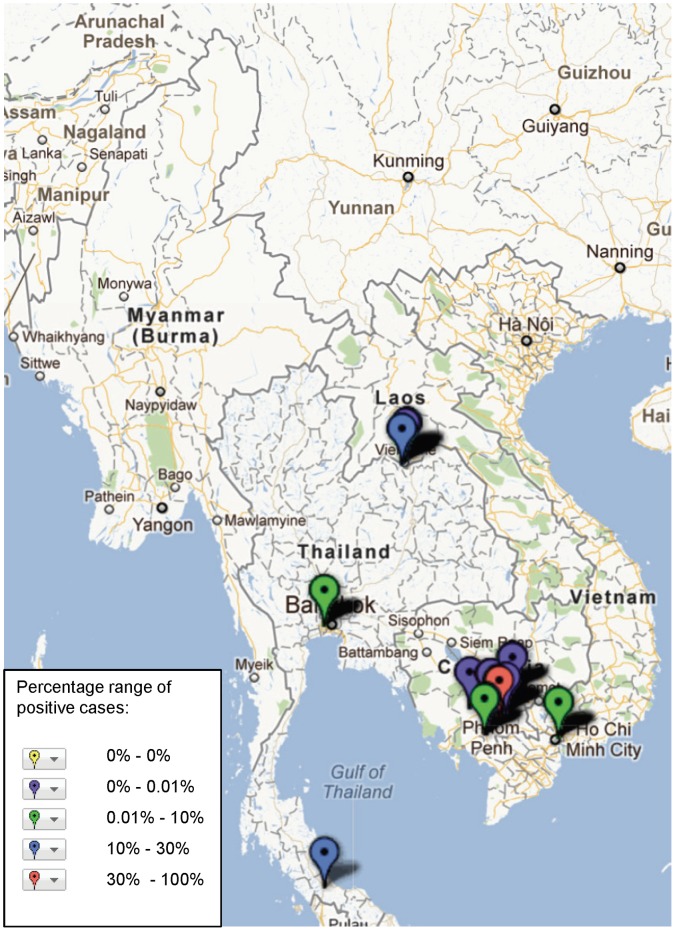
Results: Data tended to be clustered around specific areas where research institutions operate, and where resources to conduct studies are greater. The most frequently reported pathogen was dengue virus (n = 70), followed by Orientia tsutsugamushi and Rickettsia species (scrub typhus/murine typhus/spotted fever group n = 58), Leptospira spp. (n = 35), Salmonella enterica serovar Typhi and Paratyphi (enteric fever n = 24), Burkholderia pseudomallei (melioidosis n = 14), and Japanese encephalitis virus (n = 18). Wide tracts with very little published data on aetiology of fever are apparent.
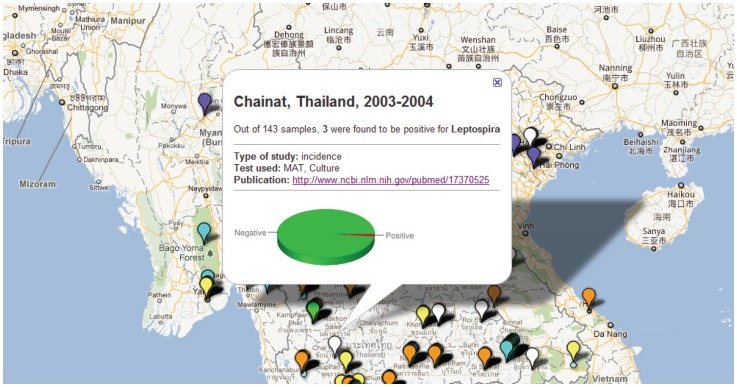
Discussion and conclusions: This mapping demonstrates a very heterogeneous distribution of information on the causes of fever in the Mekong countries. Further directed data collection to address gaps in the evidence-base, and expansion to a global database of pathogen distribution, is readily achievable, and would help define wider priorities for research and development to improve syndromic management of fever, prioritize diagnostic development, and guide empirical therapy.
Conflict of interest statement
Figures
References
-
- United Nations (2010) The Millennium Development Goals Report 2010. New York: United Nations.
-
- WHO (2010) World Malaria Report 2010. Geneva: World Health Organization.
-
- WHO (2010) Guidelines for the treatment of malaria, 2nd edition Geneva: World Health Organization. - PubMed
-
- Black RE, Cousens S, Johnson HL, Lawn JE, Rudan I, et al.. (2010) Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet: 11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
