

Inflammation, coagulation and cardiovascular disease in HIV-infected individuals
- PMID: 22970224
- PMCID: PMC3438173
- DOI: 10.1371/journal.pone.0044454
Inflammation, coagulation and cardiovascular disease in HIV-infected individuals
Abstract
Background: The SMART study was a trial of intermittent use of antiretroviral therapy (ART) (drug conservation [DC]) versus continuous use of ART (viral suppression [VS]) as a strategy to reduce toxicities, including cardiovascular disease (CVD) risk. We studied the predictive value of high sensitivity C-reactive protein (hsCRP), interleukin-6 (IL-6) and D-dimer with CVD morbidity and mortality in HIV-infected patients who were enrolled in SMART beyond other measured CVD risk factors.
Methods: A blood sample was available in 5098 participants who were enrolled in the SMART study for the measurement of IL-6, hsCRP and D-dimer. Hazard ratios (HR) with 95% CI for CVD events were estimated for each quartile (Q) for each biomarker vs the 1(st) quartile and for 1 SD higher levels. For both treatment groups combined, unadjusted and adjusted HRs were determined using Cox regression models.
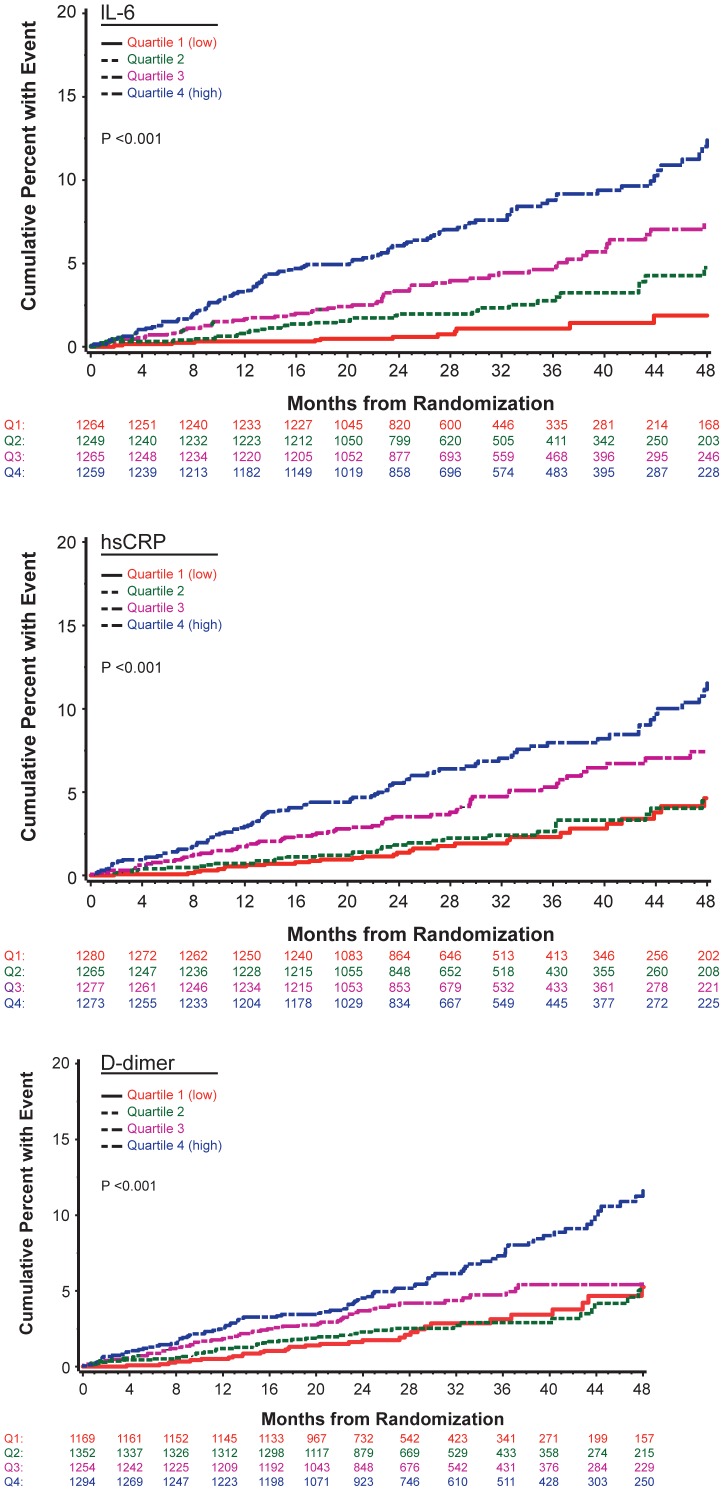
Results: There were 252 participants who had a CVD event over a median follow-up of 29 months. Adjusted HRs (95% CI) for CVD for Q4 vs Q1 were 4.65 (2.61, 8.29), 2.10 (1.40, 3.16), and 2.14 (1.38, 3.33) for IL-6, hsCRP and D-dimer, respectively. Associations were similar for the DC and VS treatment groups (interaction p-values were >0.30). The addition of the three biomarkers to a model that included baseline covariates significantly improved model fit (p<0.001). Area under the curve (AUC) estimates improved with inclusion of the three biomarkers in a model that included baseline covariates corresponding to other CVD risk factors and HIV factors (0.741 to 0.771; p<0.001 for difference).
Conclusions: In HIV-infected individuals, IL-6, hsCRP and D-dimer are associated with an increased risk of CVD independent of other CVD risk factors. Further research is needed to determine whether these biomarkers can be used to improve CVD risk prediction among HIV positive individuals.
Conflict of interest statement
Figures

References
-
- Hogg RS, Heath KV, Yip B, Craib KJ, O’Shaughnessy MV, et al. (1998) Improved survival among HIV-infected individuals following initiation of antiretroviral therapy. JAMA 279(6): 450–454. - PubMed
-
- Mocroft A, Ledergerber B, Katlama C, Kirk O, Reiss P, et al. (2003) Decline in AIDS and death rates in the EuroSIDA study: an observational study. Lancet 362(9377): 22–29. - PubMed
-
- Calmy A, Hirschel B, Cooper DA, Carr A (2009) A new era of antiretroviral drug toxicity. Antivir Ther 14(2): 165–179. - PubMed
-
- DAD Study Group, Friis-Moller N, Reiss P, Sabin CA, Weber R, et al (2007) Class of antiretroviral drugs of myocardial infarction. N Engl J Med 356(17): 1723–1735. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
