

Bicuspid aortic valve and thoracic aortic aneurysm: three patient populations, two disease phenotypes, and one shared genotype
- PMID: 22970404
- PMCID: PMC3434382
- DOI: 10.1155/2012/926975
Bicuspid aortic valve and thoracic aortic aneurysm: three patient populations, two disease phenotypes, and one shared genotype
Abstract
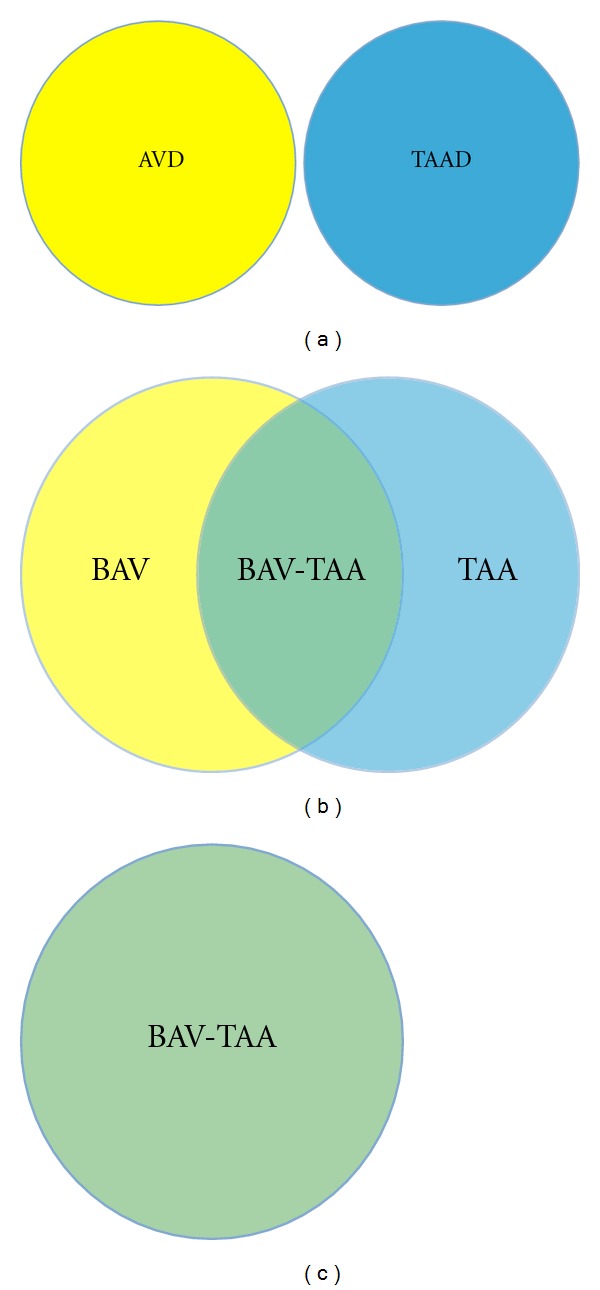
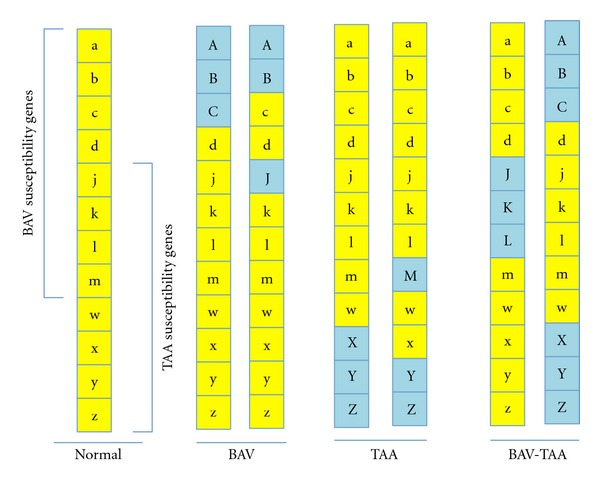
Bicuspid aortic valve (BAV) and thoracic aortic aneurysm (TAA) are two discrete cardiovascular phenotypes characterized by latent progressive disease states. There is a clear association between BAV and TAA; however the nature and extent of this relationship is unclear. There are both distinct and overlapping developmental pathways that have been established to contribute to the formation of the aortic valve and the aortic root, and the mature anatomy of these different tissue types is intimately intertwined. Likewise, human genetics studies have established apparently separate and common contributions to these clinical phenotypes, suggesting complex inheritance and a shared genetic basis and translating 3 patient populations, namely, BAV, TAA, or both, into a common but diverse etiology. A better understanding of the BAV-TAA association will provide an opportunity to leverage molecular information to modify clinical care through more sophisticated diagnostic testing, improved counseling, and ultimately new pharmacologic therapies.
Figures


Similar articles
-
Focus on the unique mechanisms involved in thoracic aortic aneurysm formation in bicuspid aortic valve versus tricuspid aortic valve patients: clinical implications of a pilot study.Eur J Cardiothorac Surg. 2013 Jun;43(6):e180-6. doi: 10.1093/ejcts/ezs630. Epub 2012 Dec 17. Eur J Cardiothorac Surg. 2013. PMID: 23248206
-
Candidate Gene Resequencing in a Large Bicuspid Aortic Valve-Associated Thoracic Aortic Aneurysm Cohort: SMAD6 as an Important Contributor.Front Physiol. 2017 Jun 13;8:400. doi: 10.3389/fphys.2017.00400. eCollection 2017. Front Physiol. 2017. PMID: 28659821 Free PMC article.
-
Copy number variation analysis in bicuspid aortic valve-related aortopathy identifies TBX20 as a contributing gene.Eur J Hum Genet. 2019 Jul;27(7):1033-1043. doi: 10.1038/s41431-019-0364-y. Epub 2019 Feb 28. Eur J Hum Genet. 2019. PMID: 30820038 Free PMC article. Clinical Trial.
-
Differential expression of MMP-2, MMP-9 and TIMP proteins in thoracic aortic aneurysm - comparison with and without bicuspid aortic valve: a meta-analysis.Vasa. 2014 Nov;43(6):433-42. doi: 10.1024/0301-1526/a000390. Vasa. 2014. PMID: 25339161 Review.
-
Managing Thoracic Aortic Aneurysm in Patients with Bicuspid Aortic Valve Based on Aortic Root-Involvement.Front Physiol. 2017 Jun 13;8:397. doi: 10.3389/fphys.2017.00397. eCollection 2017. Front Physiol. 2017. PMID: 28659818 Free PMC article. Review.
Cited by
-
Experimental evidence of the genetic hypothesis on the etiology of bicuspid aortic valve aortopathy in the hamster model.Front Cardiovasc Med. 2022 Aug 8;9:928362. doi: 10.3389/fcvm.2022.928362. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36003906 Free PMC article.
-
Bicuspid Aortic Valve: a Review with Recommendations for Genetic Counseling.J Genet Couns. 2016 Dec;25(6):1171-1178. doi: 10.1007/s10897-016-0002-6. Epub 2016 Aug 22. J Genet Couns. 2016. PMID: 27550231 Free PMC article. Review.
-
New Insights Into Aortic Diseases: A Report From the Third International Meeting on Aortic Diseases (IMAD3).Aorta (Stamford). 2013 Jun 1;1(1):23-39. doi: 10.12945/j.aorta.2013.13.006. eCollection 2013 Jun. Aorta (Stamford). 2013. PMID: 26798669 Free PMC article.
-
TGF-β mediates early angiogenesis and latent fibrosis in an Emilin1-deficient mouse model of aortic valve disease.Dis Model Mech. 2014 Aug;7(8):987-96. doi: 10.1242/dmm.015255. Dis Model Mech. 2014. PMID: 25056700 Free PMC article.
-
Review of molecular and mechanical interactions in the aortic valve and aorta: implications for the shared pathogenesis of aortic valve disease and aortopathy.J Cardiovasc Transl Res. 2014 Dec;7(9):823-46. doi: 10.1007/s12265-014-9602-4. Epub 2014 Nov 20. J Cardiovasc Transl Res. 2014. PMID: 25410134 Review.
References
-
- Hoffman JIE, Kaplan S. The incidence of congenital heart disease. Journal of the American College of Cardiology. 2002;39(12):1890–1900. - PubMed
-
- Roberts WC. The congenitally bicuspid aortic valve. A study of 85 autopsy cases. The American Journal of Cardiology. 1970;26(1):72–83. - PubMed
-
- Roberts WC, Ko JM. Frequency by decades of unicuspid, bicuspid, and tricuspid aortic valves in adults having isolated aortic valve replacement for aortic stenosis, with or without associated aortic regurgitation. Circulation. 2005;111(7):920–925. - PubMed
-
- Rajamannan NM, Bonow RO, Rahimtoola SH. Calcific aortic stenosis: an update. Nature Clinical Practice Cardiovascular Medicine. 2007;4(5):254–262. - PubMed
LinkOut - more resources
Full Text Sources