

Classification of positive blood cultures: computer algorithms versus physicians' assessment--development of tools for surveillance of bloodstream infection prognosis using population-based laboratory databases
- PMID: 22970812
- PMCID: PMC3546010
- DOI: 10.1186/1471-2288-12-139
Classification of positive blood cultures: computer algorithms versus physicians' assessment--development of tools for surveillance of bloodstream infection prognosis using population-based laboratory databases
Abstract
Background: Information from blood cultures is utilized for infection control, public health surveillance, and clinical outcome research. This information can be enriched by physicians' assessments of positive blood cultures, which are, however, often available from selected patient groups or pathogens only. The aim of this work was to determine whether patients with positive blood cultures can be classified effectively for outcome research in epidemiological studies by the use of administrative data and computer algorithms, taking physicians' assessments as reference.
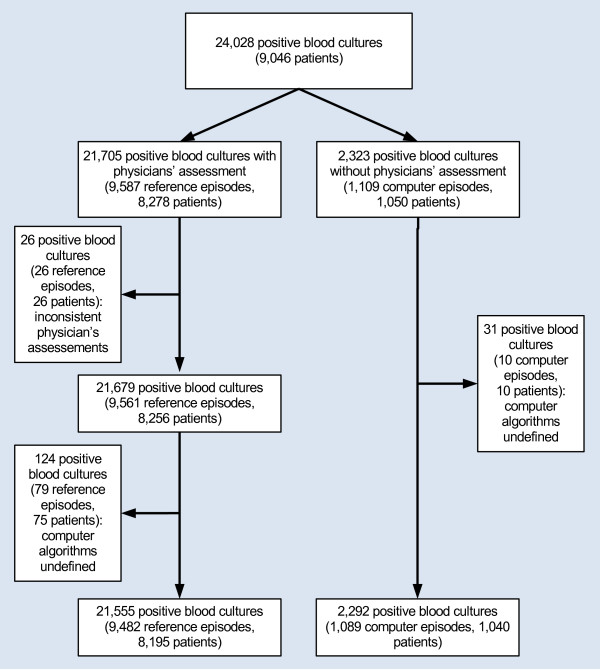
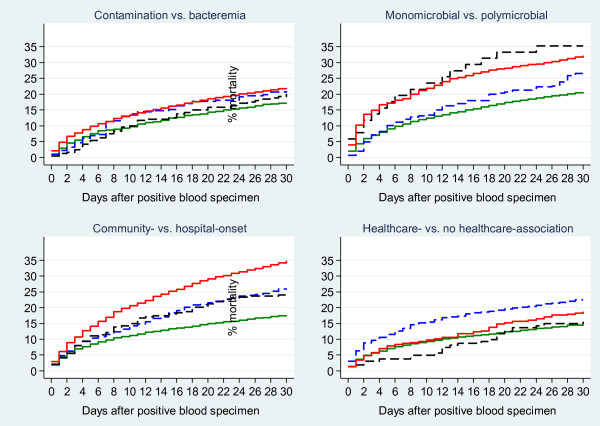
Methods: Physicians' assessments of positive blood cultures were routinely recorded at two Danish hospitals from 2006 through 2008. The physicians' assessments classified positive blood cultures as: a) contamination or bloodstream infection; b) bloodstream infection as mono- or polymicrobial; c) bloodstream infection as community- or hospital-onset; d) community-onset bloodstream infection as healthcare-associated or not. We applied the computer algorithms to data from laboratory databases and the Danish National Patient Registry to classify the same groups and compared these with the physicians' assessments as reference episodes. For each classification, we tabulated episodes derived by the physicians' assessment and the computer algorithm and compared 30-day mortality between concordant and discrepant groups with adjustment for age, gender, and comorbidity.
Results: Physicians derived 9,482 reference episodes from 21,705 positive blood cultures. The agreement between computer algorithms and physicians' assessments was high for contamination vs. bloodstream infection (8,966/9,482 reference episodes [96.6%], Kappa = 0.83) and mono- vs. polymicrobial bloodstream infection (6,932/7,288 reference episodes [95.2%], Kappa = 0.76), but lower for community- vs. hospital-onset bloodstream infection (6,056/7,288 reference episodes [83.1%], Kappa = 0.57) and healthcare-association (3,032/4,740 reference episodes [64.0%], Kappa = 0.15). The 30-day mortality in the discrepant groups differed from the concordant groups as regards community- vs. hospital-onset, whereas there were no material differences within the other comparison groups.
Conclusions: Using data from health administrative registries, we found high agreement between the computer algorithms and the physicians' assessments as regards contamination vs. bloodstream infection and monomicrobial vs. polymicrobial bloodstream infection, whereas there was only moderate agreement between the computer algorithms and the physicians' assessments concerning the place of onset. These results provide new information on the utility of computer algorithms derived from health administrative registries.
Figures
Similar articles
-
The Danish Collaborative Bacteraemia Network (DACOBAN) database.Clin Epidemiol. 2014 Sep 18;6:301-8. doi: 10.2147/CLEP.S66998. eCollection 2014. Clin Epidemiol. 2014. PMID: 25258557 Free PMC article. Review.
-
Development of a novel electronic surveillance system for monitoring of bloodstream infections.Infect Control Hosp Epidemiol. 2010 Jul;31(7):740-7. doi: 10.1086/653207. Infect Control Hosp Epidemiol. 2010. PMID: 20470039
-
National Automated Surveillance of Hospital-Acquired Bacteremia in Denmark Using a Computer Algorithm.Infect Control Hosp Epidemiol. 2017 May;38(5):559-566. doi: 10.1017/ice.2017.1. Epub 2017 Mar 9. Infect Control Hosp Epidemiol. 2017. PMID: 28274300
-
National Bloodstream Infection Surveillance in Switzerland 2008-2014: Different Patterns and Trends for University and Community Hospitals.Infect Control Hosp Epidemiol. 2016 Sep;37(9):1060-7. doi: 10.1017/ice.2016.137. Epub 2016 Jun 28. Infect Control Hosp Epidemiol. 2016. PMID: 27350313
-
Increasing bacteremia due to coagulase-negative staphylococci: fiction or reality?Infect Control Hosp Epidemiol. 1998 Aug;19(8):581-9. doi: 10.1086/647878. Infect Control Hosp Epidemiol. 1998. PMID: 9758060 Review.
Cited by
-
Effect of socioeconomic status on mortality after bacteremia in working-age patients. A Danish population-based cohort study.PLoS One. 2013 Jul 25;8(7):e70082. doi: 10.1371/journal.pone.0070082. Print 2013. PLoS One. 2013. PMID: 23936145 Free PMC article.
-
Population-based epidemiology and microbiology of community-onset bloodstream infections.Clin Microbiol Rev. 2014 Oct;27(4):647-64. doi: 10.1128/CMR.00002-14. Clin Microbiol Rev. 2014. PMID: 25278570 Free PMC article. Review.
-
The Danish Collaborative Bacteraemia Network (DACOBAN) database.Clin Epidemiol. 2014 Sep 18;6:301-8. doi: 10.2147/CLEP.S66998. eCollection 2014. Clin Epidemiol. 2014. PMID: 25258557 Free PMC article. Review.
-
How do bacteraemic patients present to the emergency department and what is the diagnostic validity of the clinical parameters; temperature, C-reactive protein and systemic inflammatory response syndrome?Scand J Trauma Resusc Emerg Med. 2014 Jul 15;22:39. doi: 10.1186/1757-7241-22-39. Scand J Trauma Resusc Emerg Med. 2014. PMID: 25027551 Free PMC article.
-
Risk and Prognosis of Bloodstream Infections among Patients on Chronic Hemodialysis: A Population-Based Cohort Study.PLoS One. 2015 Apr 24;10(4):e0124547. doi: 10.1371/journal.pone.0124547. eCollection 2015. PLoS One. 2015. PMID: 25910221 Free PMC article.
References
-
- Weinstein MP, Reller LB, Murphy JR, Lichtenstein KA. The clinical significance of positive blood cultures: a comprehensive analysis of 500 episodes of bacteremia and fungemia in adults. I. Laboratory and epidemiologic observations. Rev Infect Dis. 1983;5:35–53. doi: 10.1093/clinids/5.1.35. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
