

Rapid transition from inhaled iloprost to inhaled treprostinil in patients with pulmonary arterial hypertension
- PMID: 22970909
- PMCID: PMC3561685
- DOI: 10.1111/1755-5922.12008
Rapid transition from inhaled iloprost to inhaled treprostinil in patients with pulmonary arterial hypertension
Abstract
Background: Inhaled treprostinil is a prostacyclin analog approved for the treatment of pulmonary arterial hypertension (PAH) that may provide a more convenient treatment option for patients receiving inhaled iloprost while maintaining the clinical benefit of inhaled prostacyclin therapy.
Aims: In this open-label safety study, 73 PAH patients were enrolled with primarily World Health Organization Class II (56%) or III (42%) symptoms. At baseline, most patients (93%) were receiving 5 μg of iloprost per dose but 38% of patients reported a dosing frequency below the labeled rate of 6-9 times daily. Patients initiated inhaled treprostinil at 3 breaths four times daily (qid) at the immediate next scheduled iloprost dose. The primary objective was to assess the safety of rapid transition from iloprost to inhaled treprostinil; clinical status and quality of life were also assessed.
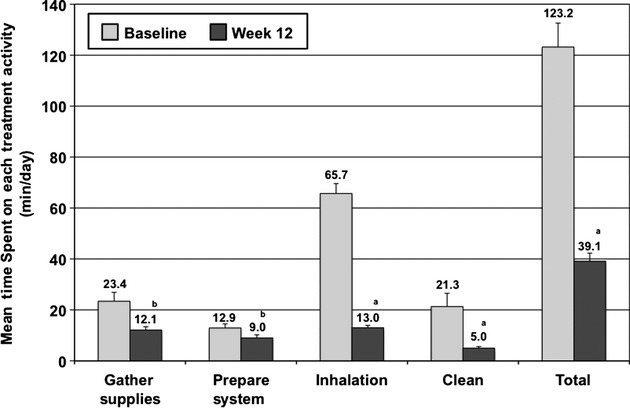
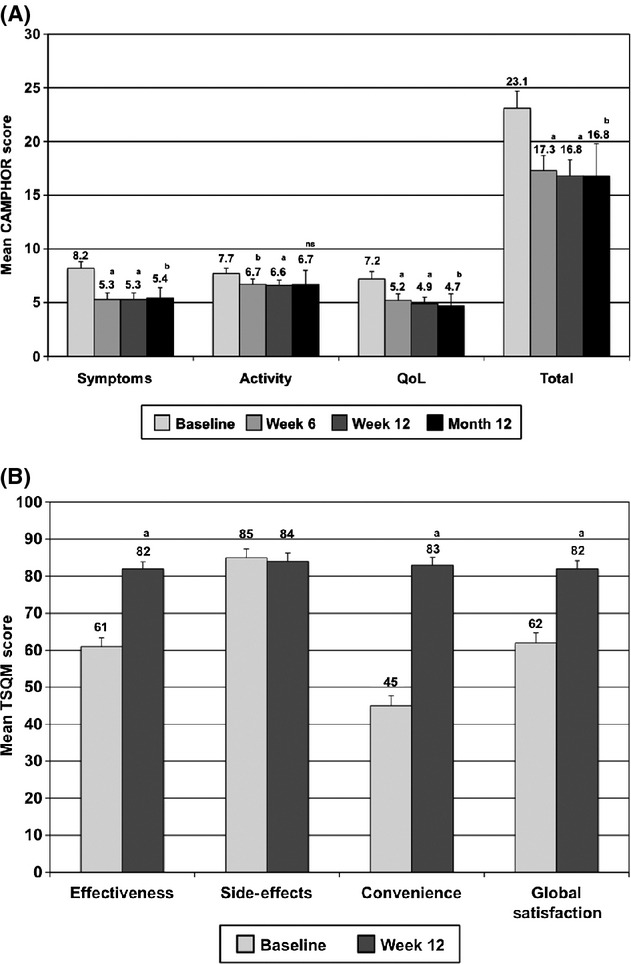
Results: Most patients (84%) achieved the target treprostinil dose of 9 breaths qid and remained on study until transition to commercial therapy (89%). The most frequent adverse events (AEs) were cough (74%), headache (44%), and nausea (30%), and five patients prematurely discontinued study drug due to AE (n = 3), disease progression (n = 1), or death (n = 1). At week 12, the time spent on daily treatment activities was reduced compared to baseline, with a mean total savings of 1.4 h per day. Improvements were also observed at week 12 for 6-min walk distance (+16.0; P < 0.001), N-terminal pro-B-type natriuretic peptide (-74 pg/mL; P = 0.001), and the Cambridge Pulmonary Hypertension Outcome Review (all domains P < 0.001).
Conclusions: Pulmonary arterial hypertension patients can be safely transitioned from inhaled iloprost to inhaled treprostinil while maintaining clinical status.
© 2012 Blackwell Publishing Ltd.
Figures
References
-
- McLaughlin VV, Archer SL, Badesch DB, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association developed in collaboration with the American College of Chest Physicians; American Thoracic Society, Inc.; and the Pulmonary Hypertension Association. J Am Coll Cardiol. 2009;53:1573–1619. - PubMed
-
- Badesch DB, McLaughlin VV, Delcroix M, et al. Prostanoid therapy for pulmonary arterial hypertension. J Am Coll Cardiol. 2004;43:56S–61S. - PubMed
-
- Barst RJ, Rubin LJ, Long WA, et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. The Primary Pulmonary Hypertension Study Group. N Engl J Med. 1996;334:296–302. - PubMed
-
- Humbert M, Morrell NW, Archer SL, et al. Cellular and molecular pathobiology of pulmonary arterial hypertension. J Am Coll Cardiol. 2004;43:13S–24S. - PubMed
-
- Humbert M, Sitbon O, Simonneau G. Treatment of pulmonary arterial hypertension. N Engl J Med. 2004;351:1425–1436. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
