

Pretreatment neutrophil-to-lymphocyte ratio in metastatic castration-resistant prostate cancer patients treated with ketoconazole: association with outcome and predictive nomogram
- PMID: 22971522
- PMCID: PMC3528383
- DOI: 10.1634/theoncologist.2012-0125
Pretreatment neutrophil-to-lymphocyte ratio in metastatic castration-resistant prostate cancer patients treated with ketoconazole: association with outcome and predictive nomogram
Abstract
Background: The neutrophil-to-lymphocyte ratio (NLR), an inflammation marker, is prognostic in several cancers. We assessed the association between the pretreatment NLR and outcome of patients with metastatic castration-resistant prostate cancer (mCRPC) treated with the CYP17 inhibitor ketoconazole.
Methods: This was an international, retrospective study of 156 mCRPC patients treated with ketoconazole. The independent effect of the pretreatment NLR and factors associated with treatment outcome were determined by multivariate analysis.
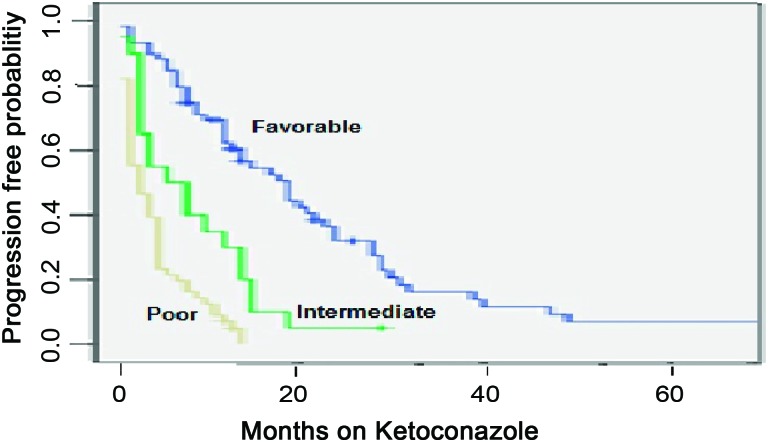
Results: Seventy-eight patients (50%) had a ≥50% decline in prostate-specific antigen (PSA). The median progression-free survival (PFS) time was 8 months. Excluded from the analysis were 23 patients without available data on their NLR and those with a recent health event or treatment associated with a blood count change. Sixty-two patients (47%) had a pretreatment NLR >3. Risk factors associated with the PFS outcome were a pretreatment NLR >3 and PSA doubling time (PSADT) <3 months and a prior response to a gonadotropin-releasing hormone agonist of <24 months or to an antiandrogen of <6 months. The number of risk factors was used to form a predictive nomogram by patient categorization into favorable (zero or one factor), intermediate (two factors), and poor (three or four factors) risk groups.
Conclusions: In mCRPC patients treated with ketoconazole, the pretreatment NLR and PSADT, and prior response to androgen-deprivation therapy, may be associated with the PFS time and used to form a risk stratification predictive nomogram.
Conflict of interest statement
Figures
Similar articles
-
Contemporary experience with ketoconazole in patients with metastatic castration-resistant prostate cancer: clinical factors associated with PSA response and disease progression.Prostate. 2012 Mar;72(4):461-7. doi: 10.1002/pros.21447. Epub 2011 Jun 17. Prostate. 2012. PMID: 21688281 Free PMC article.
-
Prostate-specific antigen doubling time predicts response to deferred antiandrogen therapy in men with androgen-independent prostate cancer.Urology. 2004 Apr;63(4):732-6. doi: 10.1016/j.urology.2003.11.016. Urology. 2004. PMID: 15072890
-
Prognostic impact of pretreatment neutrophil-to-lymphocyte ratio in castration-resistant prostate cancer patients treated with first-line docetaxel.Acta Oncol. 2017 Apr;56(4):555-562. doi: 10.1080/0284186X.2016.1260772. Epub 2017 Jan 9. Acta Oncol. 2017. PMID: 28068151
-
Safety and efficacy of maintenance therapy with a nonspecific cytochrome P17 inhibitor (CYP17i) after response/stabilization to docetaxel in metastatic castration-resistant prostate cancer.Clin Genitourin Cancer. 2013 Jun;11(2):78-84. doi: 10.1016/j.clgc.2012.11.003. Epub 2012 Dec 21. Clin Genitourin Cancer. 2013. PMID: 23260990
-
The treatment of advanced prostate cancer with ketoconazole: safety issues.Drug Saf. 1999 May;20(5):451-8. doi: 10.2165/00002018-199920050-00005. Drug Saf. 1999. PMID: 10348095 Review.
Cited by
-
Pre-radiotherapy systemic immune inflammation index associated with overall survival in patients with advanced EGFR mutant non-small cell lung cancer receiving thoracic radiotherapy.Clin Transl Oncol. 2023 Jan;25(1):226-235. doi: 10.1007/s12094-022-02936-2. Epub 2022 Sep 7. Clin Transl Oncol. 2023. PMID: 36070068 Free PMC article.
-
Validation of the neutrophil-to-lymphocyte ratio as a prognostic factor in a cohort of European prostate cancer patients.World J Urol. 2015 Nov;33(11):1661-7. doi: 10.1007/s00345-015-1494-7. Epub 2015 Jan 24. World J Urol. 2015. PMID: 25617235
-
The neutrophil-lymphocyte ratio and its utilisation for the management of cancer patients in early clinical trials.Br J Cancer. 2015 Mar 31;112(7):1157-65. doi: 10.1038/bjc.2015.67. Br J Cancer. 2015. PMID: 25719834 Free PMC article.
-
Prognostic value of selected preoperative inflammation-based scores in patients with high-risk localized prostate cancer who underwent radical prostatectomy.Onco Targets Ther. 2018 Aug 3;11:4551-4558. doi: 10.2147/OTT.S151314. eCollection 2018. Onco Targets Ther. 2018. PMID: 30122947 Free PMC article.
-
Persistent Neutrophil to Lymphocyte Ratio >3 during Treatment with Enzalutamide and Clinical Outcome in Patients with Castration-Resistant Prostate Cancer.PLoS One. 2016 Jul 19;11(7):e0158952. doi: 10.1371/journal.pone.0158952. eCollection 2016. PLoS One. 2016. PMID: 27434372 Free PMC article.
References
-
- Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Loblaw DA, Virgo KS, Nam R, et al. Initial hormonal management of androgen-sensitive metastatic, recurrent, or progressive prostate cancer: 2006 update of an American Society of Clinical Oncology practice guideline. J Clin Oncol. 2007;25:1596–1605. - PubMed
-
- Eisenberger MA, Blumenstein BA, Crawford ED, et al. Bilateral orchiectomy with or without flutamide for metastatic prostate cancer. N Engl J Med. 1998;339:1036–1042. - PubMed
-
- Reid AH, Attard G, Barrie E, et al. CYP17 inhibition as a hormonal strategy for prostate cancer. Nat Clin Pract Urol. 2008;5:610–620. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
