

Hyperoxia is associated with increased mortality in patients treated with mild therapeutic hypothermia after sudden cardiac arrest
- PMID: 22971589
- PMCID: PMC3502652
- DOI: 10.1097/CCM.0b013e3182656976
Hyperoxia is associated with increased mortality in patients treated with mild therapeutic hypothermia after sudden cardiac arrest
Abstract
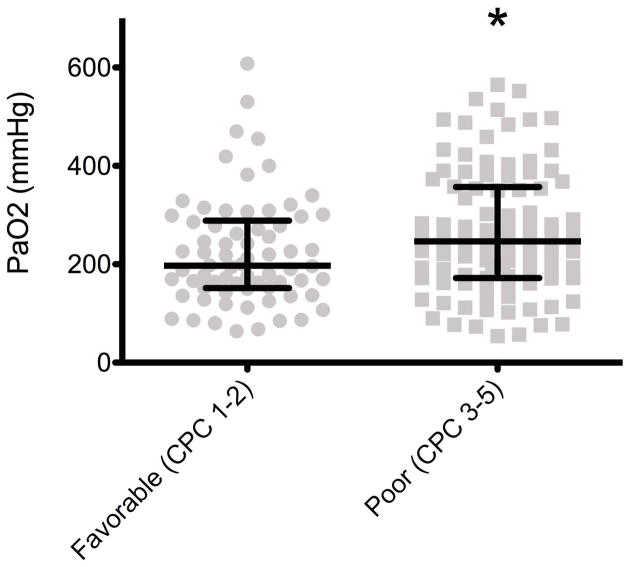
Objective: To determine whether higher levels of PaO2 are associated with in-hospital mortality and poor neurological status at hospital discharge in patients treated with mild therapeutic hypothermia after sudden cardiac arrest.
Design: Retrospective analysis of a prospective cohort.
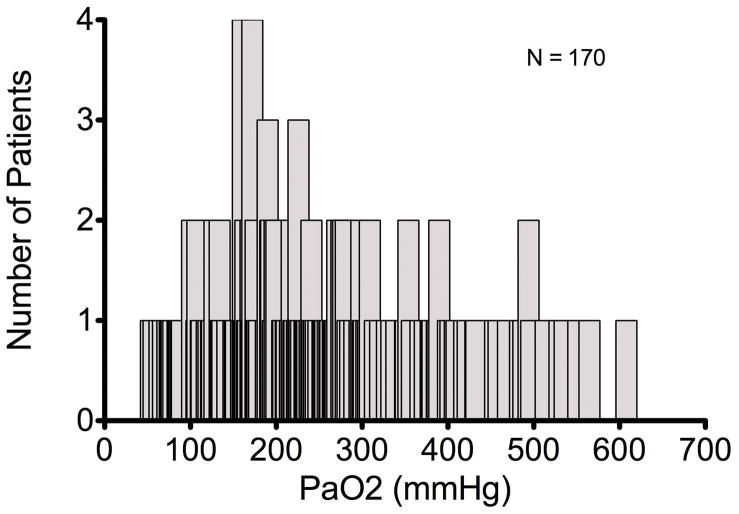
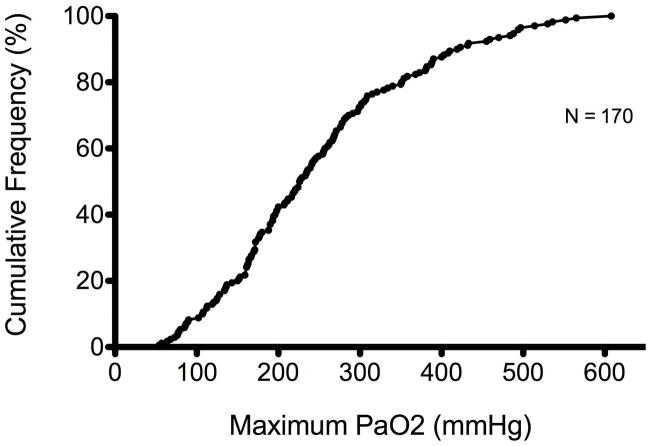
Patients: A total of 170 consecutive patients treated with therapeutic hypothermia in the cardiovascular care unit of an academic tertiary care hospital.
Interventions: None.
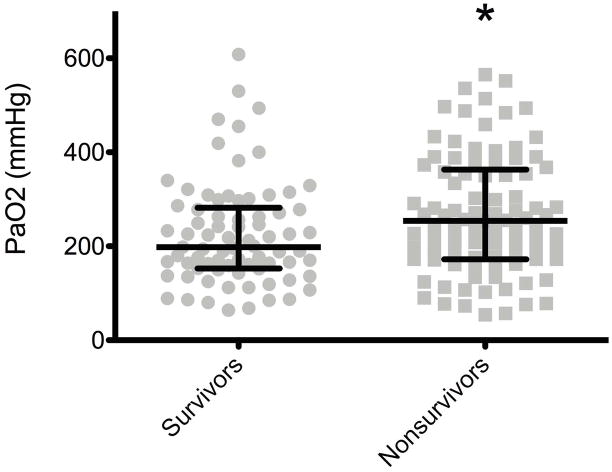
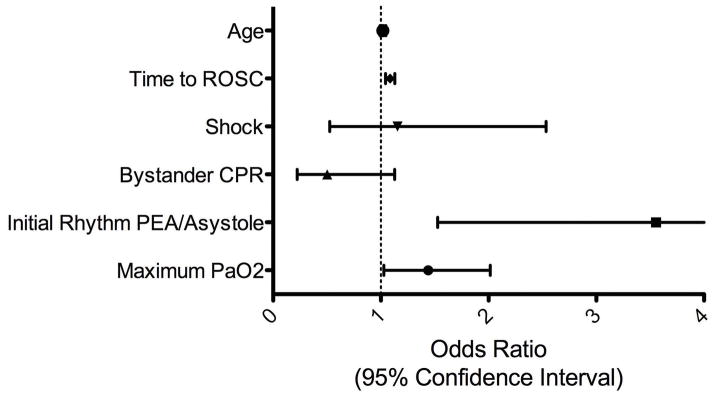
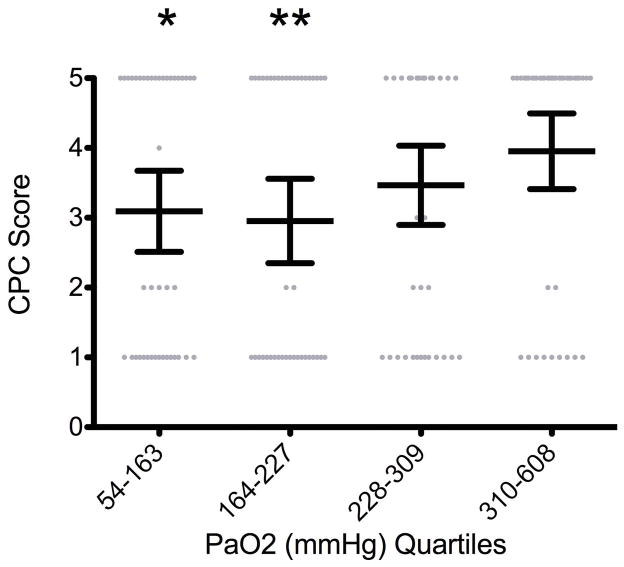
Measurements and main results: Of 170 patients, 77 (45.2%) survived to hospital discharge. Survivors had a significantly lower maximum PaO2 (198 mm Hg; interquartile range, 152.5-282) measured in the first 24 hrs following cardiac arrest compared to nonsurvivors (254 mm Hg; interquartile range, 172-363; p = .022). A multivariable analysis including age, time to return of spontaneous circulation, the presence of shock, bystander cardiopulmonary resuscitation, and initial rhythm revealed that higher levels of PaO2 were significantly associated with increased in-hospital mortality (odds ratio 1.439; 95% confidence interval 1.028-2.015; p = .034) and poor neurological status at hospital discharge (odds ratio 1.485; 95% confidence interval 1.032-2.136; p = .033).
Conclusions: Higher levels of the maximum measured PaO2 are associated with increased in-hospital mortality and poor neurological status on hospital discharge in patients treated with mild therapeutic hypothermia after sudden cardiac arrest.
Conflict of interest statement
The authors have not disclosed any potential conflicts of interest
The authors declare that they have no conflicts of interest.
Figures
Comment in
-
Postresuscitation treatment targets-time to emphasize normoxia?Crit Care Med. 2012 Dec;40(12):3306-7. doi: 10.1097/CCM.0b013e318270e715. Crit Care Med. 2012. PMID: 23164770 No abstract available.
References
-
- Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests from the national registry of cardiopulmonary resuscitation. Resuscitation. 2003;58:297–308. - PubMed
-
- Stiel IG, Wells GA, Field B, et al. Advanced cardiac life support in out-of-hospital cardiac arrest. N Engl J Med. 2004;351:647–656. - PubMed
-
- Bernard SA, Gray TW, Busted, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–563. - PubMed
-
- Hypothermia After Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549–556. - PubMed
-
- Nolan JP, Morley TL, Vanden Hoek RW, et al. Therapeutic hypothermia after cardiac arrest: an advisory statement by the advanced life support task force of the international liaison committee on resuscitation. Circulation. 2003;108:118–121. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
