

Early amniotomy and early oxytocin for prevention of, or therapy for, delay in first stage spontaneous labour compared with routine care
- PMID: 22972098
- PMCID: PMC4160792
- DOI: 10.1002/14651858.CD006794.pub3
Early amniotomy and early oxytocin for prevention of, or therapy for, delay in first stage spontaneous labour compared with routine care
Update in
-
Early amniotomy and early oxytocin for prevention of, or therapy for, delay in first stage spontaneous labour compared with routine care.Cochrane Database Syst Rev. 2013 Aug 7;2013(8):CD006794. doi: 10.1002/14651858.CD006794.pub4. Cochrane Database Syst Rev. 2013. PMID: 23926074 Free PMC article.
Abstract
Background: Caesarean section rates are over 20% in many developed countries. The main diagnosis contributing to the high rate in nulliparae is dystocia or prolonged labour. The present review assesses the effects of a policy of early amniotomy with early oxytocin administration for the prevention of, or the therapy for, delay in labour progress.
Objectives: To estimate the effects of early augmentation with amniotomy and oxytocin for prevention of, or therapy for, delay in labour progress on the caesarean birth rate and on indicators of maternal and neonatal morbidity.
Search methods: We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (15 February 2012), MEDLINE (1966 to 15 February 2012), EMBASE (1980 to 15 February 2012), CINAHL (1982 to 15 February 2012), MIDIRS (1985 to February 2012) and contacted authors for data from unpublished trials.
Selection criteria: Randomized and quasi-randomized controlled trials that compared oxytocin and amniotomy with expectant management.
Data collection and analysis: Three review authors extracted data independently. We stratified the analyses into 'Prevention Trials' and 'Therapy Trials' according to the status of the woman at the time of randomization. Participants in the 'Prevention Trials' were unselected women, without slow progress in labour, who were randomized to a policy of early augmentation or to routine care. In 'Treatment Trials' women were eligible if they had an established delay in labour progress.
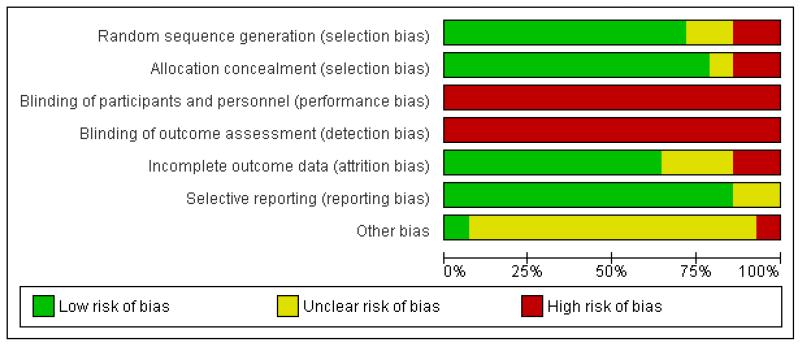
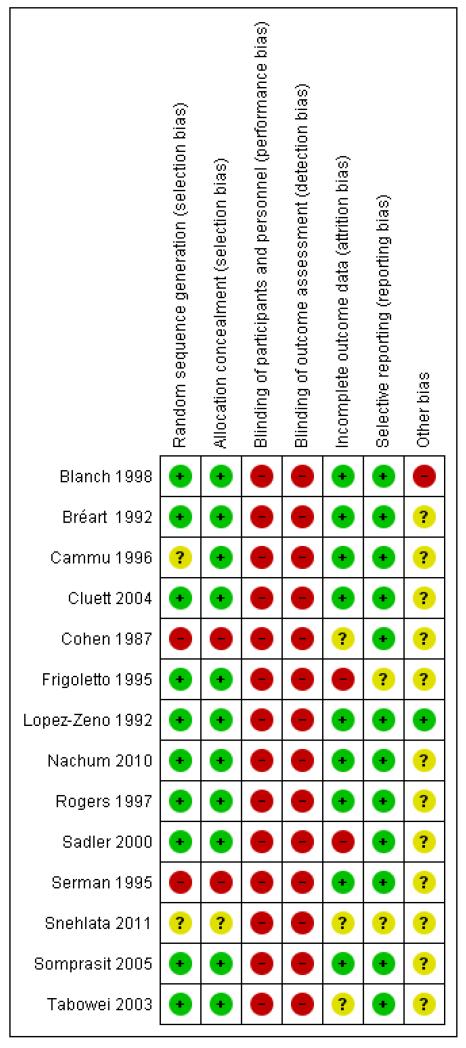
Main results: For this update, we have included a further two new clinical trials. This updated review includes 14 trials, randomizing a total of 8033 women. The unstratified analysis found early intervention with amniotomy and oxytocin to be associated with a modest reduction in the risk of caesarean section; however, the confidence interval (CI) included the null effect (risk ratio (RR) 0.89; 95% CI 0.79 to 1.01; 14 trials; 8033 women). In prevention trials, early augmentation was associated with a modest reduction in the number of caesarean births (RR 0.87; 95% CI 0.77 to 0.99; 11 trials; 7753). A policy of early amniotomy and early oxytocin was associated with a shortened duration of labour (average mean difference (MD) - 1.28 hours; 95% CI -1.97 to -0.59; eight trials; 4816 women). Sensitivity analyses excluding four trials with a full package of active management did not substantially affect the point estimate for risk of caesarean section (RR 0.87; 95% CI 0.73 to 1.05; 10 trials; 5165 women). We found no other significant effects for the other indicators of maternal or neonatal morbidity.
Authors' conclusions: In prevention trials, early intervention with amniotomy and oxytocin appears to be associated with a modest reduction in the rate of caesarean section over standard care.
Figures
Update of
-
Early amniotomy and early oxytocin for prevention of, or therapy for, delay in first stage spontaneous labour compared with routine care.Cochrane Database Syst Rev. 2009 Apr 15;(2):CD006794. doi: 10.1002/14651858.CD006794.pub2. Cochrane Database Syst Rev. 2009. Update in: Cochrane Database Syst Rev. 2012 Sep 12;(9):CD006794. doi: 10.1002/14651858.CD006794.pub3. PMID: 19370654 Updated.
References
References to studies included in this review
-
- Blanch G, Walkinshaw S, Alfirevic Z. Dysfunctional labour: a randomised trial. British Journal of Obstetrics and Gynaecology. 1998;105:117–20. - PubMed
-
- Bréart G, Du Mazaubrun C, Maillard F, Garel M. Comparison of two policies of management of labour for primiparous women: effects of early rupture of membranes and use of oxytocin. Results of randomized controlled trial; Proceedings of International Conference on Primary Care, Obstetrics and Perinatal Health; Utrecht, Netherlands. 1991; p. 49. 1991.
-
- Bréart G, Garel M, Mlika-Cabanne N. Evaluation of different policies of management of labour for primiparous women. Trial A: Results of the early amniotomy trial. In: Kaminski M, editor. Evaluation in pre-, peri-, and postnatal care delivery systems. INSERM; Paris: 1992. pp. 43–56.
-
- Breart G, Mlika-Cabane N, Kaminski M, Alexander S, Herruzo-Nalda A, Mandruzzato P, et al. Evaluation of different policies for the management of labour. Early Human Development. 1992;29(1):309–12. - PubMed
-
*
-
- Breart G, Mlika-Cabanne N, Kaminski M. The evaluation of different policies for the management of labour: Trial A. Results of the early amniotomy trial; Proceedings of 3rd European Health Services Research Meeting; London, UK. 1991; 1991.
References to studies excluded from this review
-
- Cardozo L, Pearce M. Oxytocin in active-phase abnormalities of labor: a randomized study. Obstetrics & Gynecology. 1990;75:152–7. - PubMed
-
*
-
- Cardozo LD. Dysfunctional labour; Proceedings of Silver Jubilee British Congress of Obstetrics and Gynaecology; London, UK. 1989 July 4-7; p. 76. 1989.
-
- Cummiskey KC, Gall SA, Dawood MY. Pulsatile administration of oxytocin for augmentation of labor. Obstetrics & Gynaecology. 1989;74:869–72. - PubMed
-
- Gagnon-Gervais K, Iglesias MH, Duperron L, Masse A, Mayrand MH, Sansregret A, et al. Early vs late amniotomy for labor induction: a randomized controlled trial. American Journal of Obstetrics and Gynecology. 2011;204(1 Suppl):S127.
-
- Hogston P, Noble W. Active management of labour - the Portsmouth experience. Journal of Obstetrics and Gynaecology. 1993;13:340–2.
Additional references
-
- Betran AP, Merialdi M, Lauer JA, Bing-Shun W, Thomas J, Van Look P, et al. Rates of caesarean section: analysis of global, regional and national estimates. Paediatric and Perinatal Epidemiology. 2007;21(2):98–113. - PubMed
-
- Bidgood KA, Steer PJ. A randomized control study of oxytocin augmentation of labour. 1. Obstetric outcome. British Journal of Obstetrics and Gynaecology. 1987;94(6):512–7. - PubMed
-
- Blanks AM, Vatish M, Allen MJ, Ladds G, de Wit NC, Slater DM, et al. Paracrine oxytocin and estradiol demonstrate a spatial increase in human intrauterine tissues with labor. Journal of Clinical Endocrinology and Metabolism. 2003;88(7):3392–400. - PubMed
References to other published versions of this review
-
- Wei S, Wo BL, Xu H, Luo ZC, Roy C, Fraser WD. Early amniotomy and early oxytocin for prevention of, or therapy for, delay in first stage spontaneous labour compared with routine care. Cochrane Database of Systematic Reviews. 2009;(2) DOI: 10.1002/14651858.CD006794.pub2. - PubMed
-
-
* Indicates the major publication for the study
-
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical