

Telephone counseling intervention improves dietary habits and metabolic parameters of patients with the metabolic syndrome: a randomized controlled trial
- PMID: 22972443
- PMCID: PMC3448172
- DOI: 10.1900/RDS.2012.9.36
Telephone counseling intervention improves dietary habits and metabolic parameters of patients with the metabolic syndrome: a randomized controlled trial
Abstract
Background: Patients with the metabolic syndrome (MetS) can suffer from poor metabolic parameters through lack of adherence to requisite lifestyle changes in dietary and physical activity. Usually, interventions in MetS patients are infrequent face-to-face consultations. The low frequency or absence of counseling interviews leads to a shortage of information and motivation to adhere to the recommended lifestyle changes. Telephone interventions could be an additional low-cost tool for effective interventions.
Aim: To evaluate the effectiveness of telephone intervention in improving lifestyle habits and metabolic parameters in MetS patients compared with similar face-to-face or a usual care interventions.
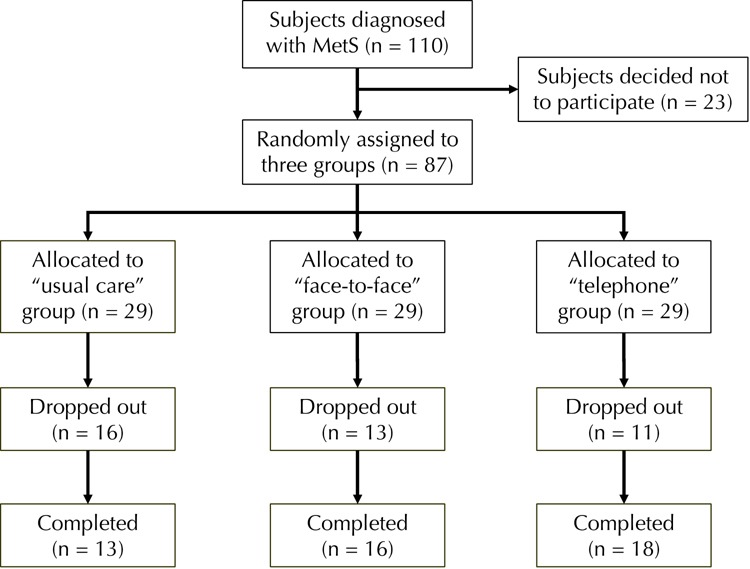
Methods: Eighty-seven MetS patients recruited from the outpatient clinic of a major public hospital were randomly assigned to one of the three intervention groups: "usual care", "telephone" or "face-to-face". At the beginning of the study, all patients were provided with a hypocaloric Mediterranean-type diet. Afterwards, patients in the telephone group received 7 dietary counseling calls, patients in the face-to-face group participated in 7 one-to-one dietary counseling sessions, while patients in the usual care group received no other contact until the end of the study, 6 months later. All patients underwent full medical and nutritional evaluation at the beginning and at the end of the intervention.
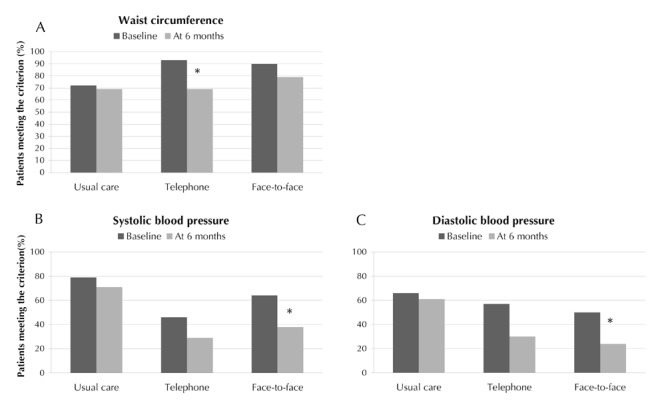
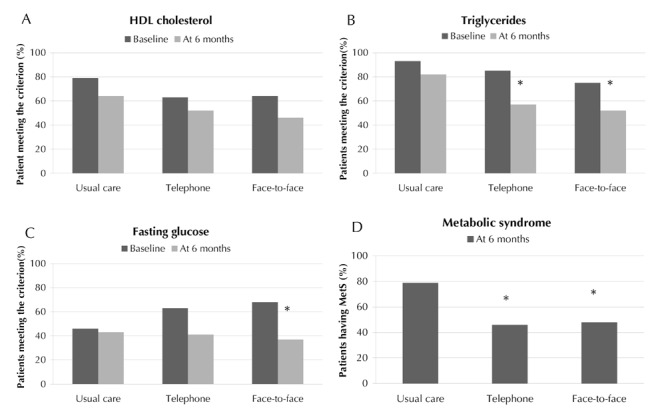
Results: At the end of the intervention, 42% of the participants no longer showed symptoms of MetS; the reduction rates differed significantly between the groups (p = 0.024), with those in the face-to-face and telephone group exhibiting similar rates (52% and 54%, respectively, vs. 21% in the usual care group). Between-group analysis revealed that the face-to-face group achieved the greatest improvement in metabolic parameters, while the telephone group had the greatest improvement in dietary adherence compared with the usual care group.
Conclusions: Telephone counseling is an effective way to implement behavioral counseling to improve lifestyle habits in MetS patients.
Figures
References
-
- King H, Aubert RE, Herman WH. Global burden of diabetes, 1995-2025: prevalence, numerical estimates, and projections. Diabetes Care. 1998;21(9):1414–1431. - PubMed
-
- Kromhout D. Epidemiology of cardiovascular diseases in Europe. Public Health Nutr. 2001;4(2B):441–457. - PubMed
-
- Darnton-Hill I, Nishida C, James WP. A life course approach to diet, nutrition and the prevention of chronic diseases. Public Health Nutr. 2004;7(1A):101–121. - PubMed
-
- Ninomiya JK, L'Italien G, Criqui MH, Whyte JL, Gamst A, Chen RS. Association of the metabolic syndrome with history of myocardial infarction and stroke in the Third National Health and Nutrition Examination Survey. Circulation. 2004;109(1):42–46. - PubMed
-
- Laaksonen DE, Lakka HM, Niskanen LK, Kaplan GA, Salonen JT, Lakka TA. Metabolic syndrome and development of diabetes mellitus: application and validation of recently suggested definitions of the metabolic syndrome in a prospective cohort study. Am J Epidemiol. 2002;156(11):1070–1077. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical