

Pediatric sarcoma in Central America: outcomes, challenges, and plans for improvement
- PMID: 22972687
- PMCID: PMC3535564
- DOI: 10.1002/cncr.27816
Pediatric sarcoma in Central America: outcomes, challenges, and plans for improvement
Abstract
Background: Children with cancer in middle-income countries have inferior outcomes compared with similar children in high-income countries. The magnitude and drivers of this survival gap are not well understood. In the current report, the authors sought to describe patterns of clinical presentation, magnitude of treatment abandonment, and survival in children with sarcoma in Central America.
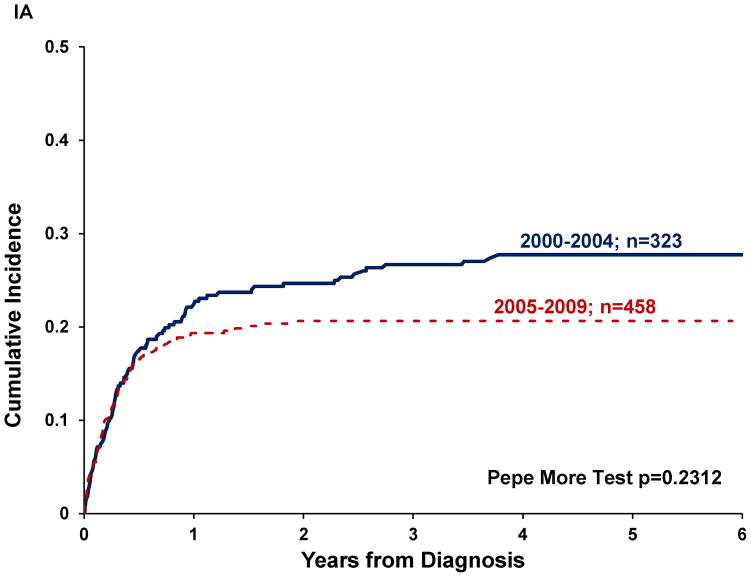
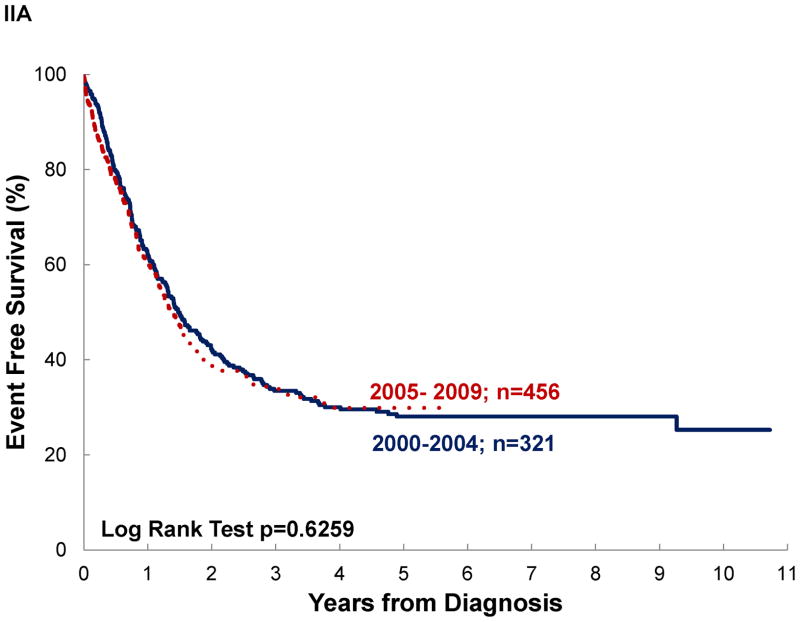
Methods: A retrospective review was conducted of hospital-based registries from national pediatric oncology referral centers. Patients with newly diagnosed osteosarcoma, Ewing sarcoma, rhabdomyosarcoma (RMS), and soft tissue sarcoma (STS) between January 1, 2000 and December 31, 2009 were included. Survival analyses were performed first using standard definitions of overall survival (OS) and event-free survival (EFS) and then with abandonment included as an event (abandonment-sensitive OS and abandonment-sensitive EFS).
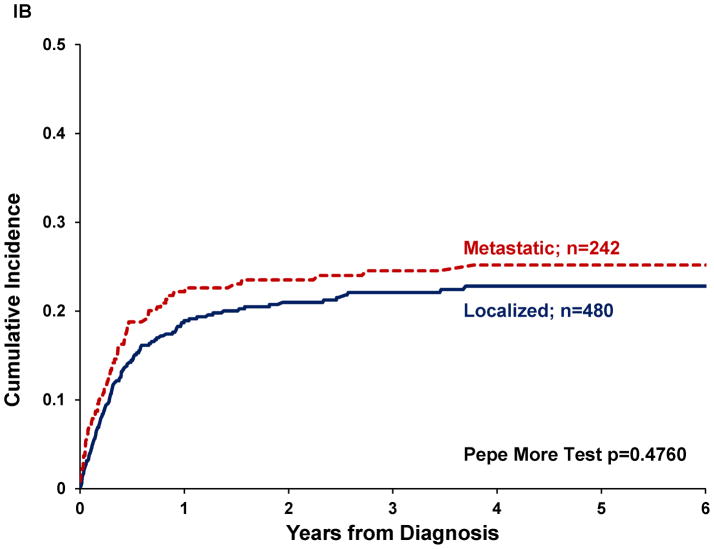
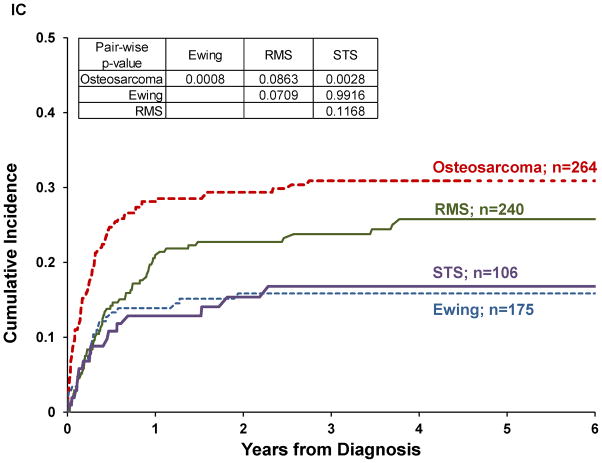
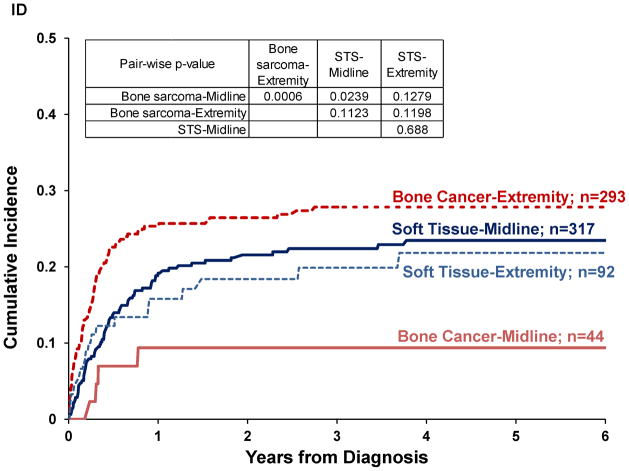
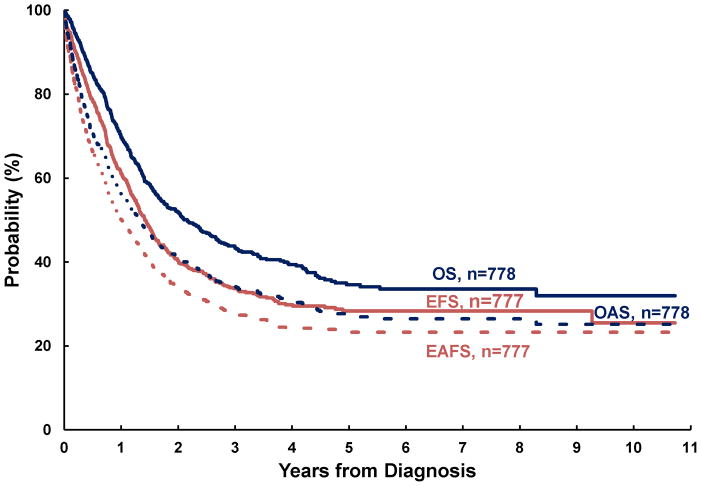
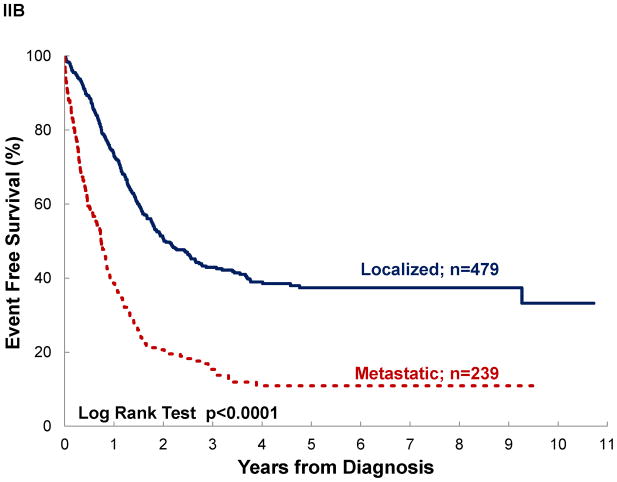
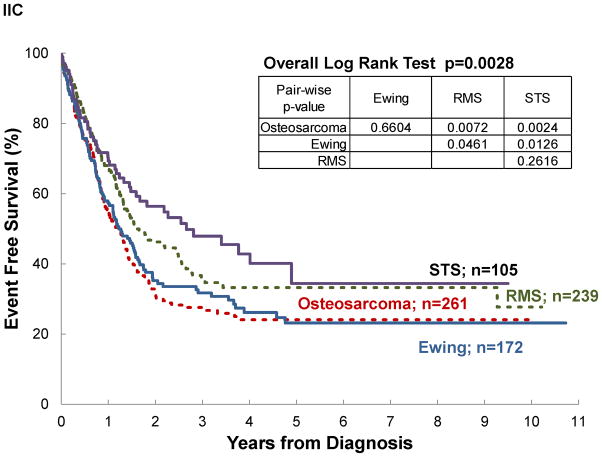
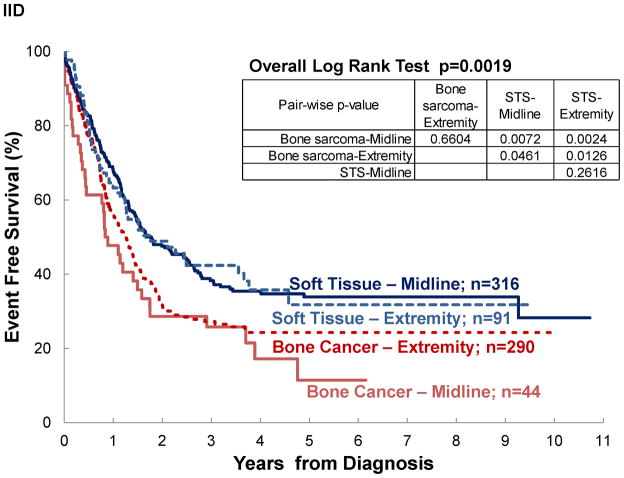
Results: In total, 785 new cases of pediatric sarcoma were reported (264 diagnoses of osteosarcoma, 175 diagnoses of Ewing sarcoma, 240 diagnoses of RMS, and 106 diagnoses of STS). The rate of metastatic disease at presentation was high (osteosarcoma, 38%; Ewing sarcoma, 39%; RMS, 29%; and STS, 21%). The treatment abandonment rate also was high, particularly among patients with extremity bone sarcomas (osteosarcoma, 30%; Ewing sarcoma, 15%; RMS, 25%; and STS, 15%). Of 559 patients who experienced a first event, 59% had either recurrent or progressive disease. The 4-year OS rate (±standard error) was 40% ± 3%, and the EFS rate was 30% ± 2%; however, these rates decreased further to 31% ± 2% and 24% ± 2%, respectively, when abandonment was taken into account.
Conclusions: The current results indicated that high rates of metastases and treatment abandonment and difficulty with upfront treatment effectiveness are important contributors to the poor survival of children with pediatric sarcomas in Central America. Initiatives for early diagnosis, psychosocial support, quality improvement, and multidisciplinary care are warranted to improve outcomes.
Copyright © 2012 American Cancer Society.
Figures
References
-
- Howard SC, Metzger ML, Wilimas JA, et al. Childhood cancer epidemiology in low-income countries. Cancer. 2008;112(3):461–72. - PubMed
-
- Kaatsch P. Epidemiology of childhood cancer. Cancer Treat Rev. 2010;36(4):277–85. - PubMed
-
- Carroll WL, Finlay JL. Cancer in children and adolescents. Sudbury, Mass: Jones and Bartlett Publishers; 2010.
-
- Tanko NM, Echejoh GO, Manasseh NA, Mandong MB, Uba AF. Paediatric solid tumours in Nigerian children: a changing pattern? Afr J Paediatr Surg. 2009;6(1):7–10. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
