

Mortality in the year following antiretroviral therapy initiation in HIV-infected adults and children in Uganda and Zimbabwe
- PMID: 22972859
- PMCID: PMC3501336
- DOI: 10.1093/cid/cis797
Mortality in the year following antiretroviral therapy initiation in HIV-infected adults and children in Uganda and Zimbabwe
Abstract
Background: Adult mortality in the first 3 months on antiretroviral therapy (ART) is higher in low-income than in high-income countries, with more similar mortality after 6 months. However, the specific patterns of changing risk and causes of death have rarely been investigated in adults, nor compared with children in low-income countries.
Methods: We used flexible parametric hazard models to investigate how mortality risks varied over the first year on ART in human immunodeficiency virus-infected adults (aged 18-73 years) and children (aged 4 months to 15 years) in 2 trials in Zimbabwe and Uganda.
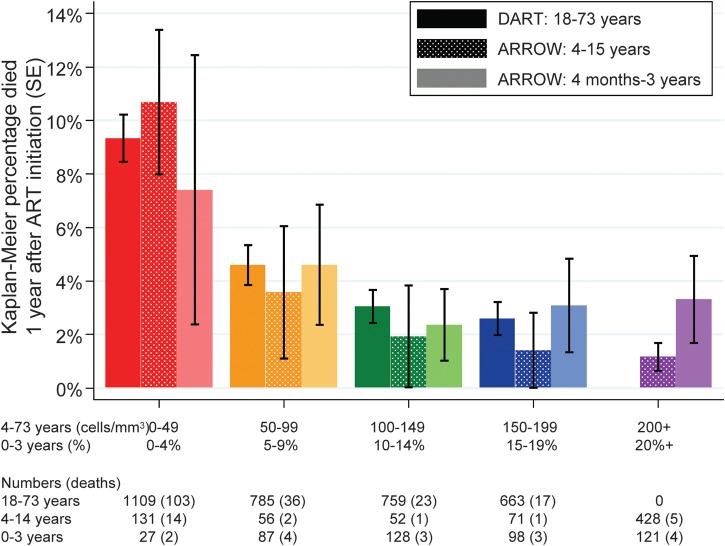
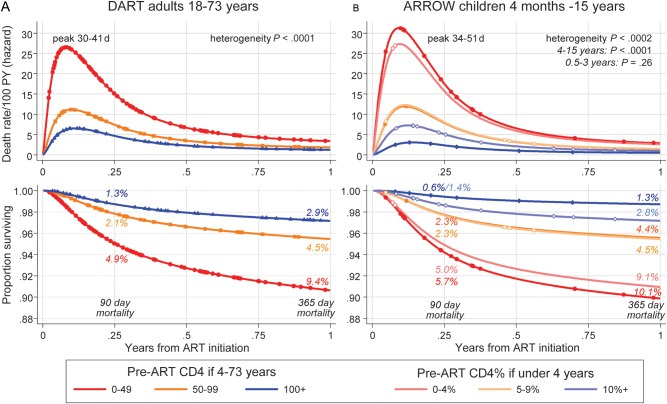
Results: One hundred seventy-nine of 3316 (5.4%) adults and 39 of 1199 (3.3%) children died; half of adult/pediatric deaths occurred in the first 3 months. Mortality variation over year 1 was similar; at all CD4 counts/CD4%, mortality risk was greatest between days 30 and 50, declined rapidly to day 180, then declined more slowly. One-year mortality after initiating ART with 0-49, 50-99 or ≥ 100 CD4 cells/μL was 9.4%, 4.5%, and 2.9%, respectively, in adults, and 10.1%, 4.4%, and 1.3%, respectively, in children aged 4-15 years. Mortality in children aged 4 months to 3 years initiating ART in equivalent CD4% strata was also similar (0%-4%: 9.1%; 5%-9%: 4.5%; ≥ 10%: 2.8%). Only 10 of 179 (6%) adult deaths and 1 of 39 (3%) child deaths were probably medication-related. The most common cause of death was septicemia/meningitis in adults (20%, median 76 days) and children (36%, median 79 days); pneumonia also commonly caused child deaths (28%, median 41 days).
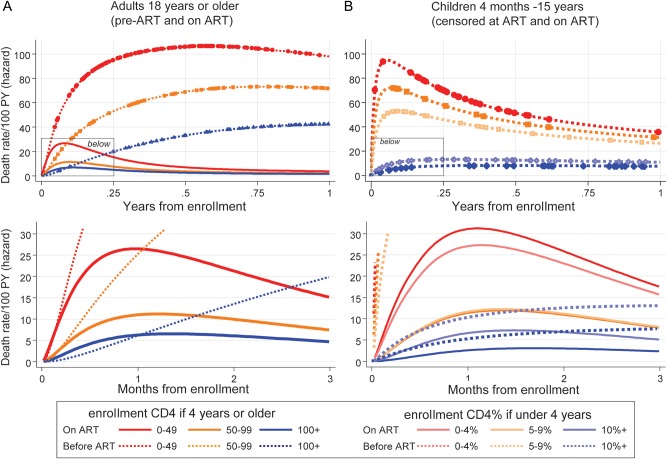
Conclusions: Children ≥ 4 years and adults with low CD4 values have remarkably similar, and high, mortality risks in the first 3 months after ART initiation in low-income countries, similar to cohorts of untreated individuals. Bacterial infections are a major cause of death in both adults and children; targeted interventions could have important benefits.
Figures
References
-
- World Health Organization. Towards universal access: scaling up priority HIV/AIDS interventions in the health sector. Progress report 2011. Geneva, Switzerland: WHO; 2011. Available at: http://whqlibdoc.who.int/publications/2011/9789241502986_eng.pdf . Accessed 18 December 2011.
-
- Braitstein P, Brinkhof MW, Dabis F, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet. 2006;367:817–24. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
