

Multiple reaction monitoring to identify site-specific troponin I phosphorylated residues in the failing human heart
- PMID: 22972900
- PMCID: PMC3733556
- DOI: 10.1161/CIRCULATIONAHA.112.096388
Multiple reaction monitoring to identify site-specific troponin I phosphorylated residues in the failing human heart
Abstract
Background: Human cardiac troponin I is known to be phosphorylated at multiple amino acid residues by several kinases. Advances in mass spectrometry allow sensitive detection of known and novel phosphorylation sites and measurement of the level of phosphorylation simultaneously at each site in myocardial samples.
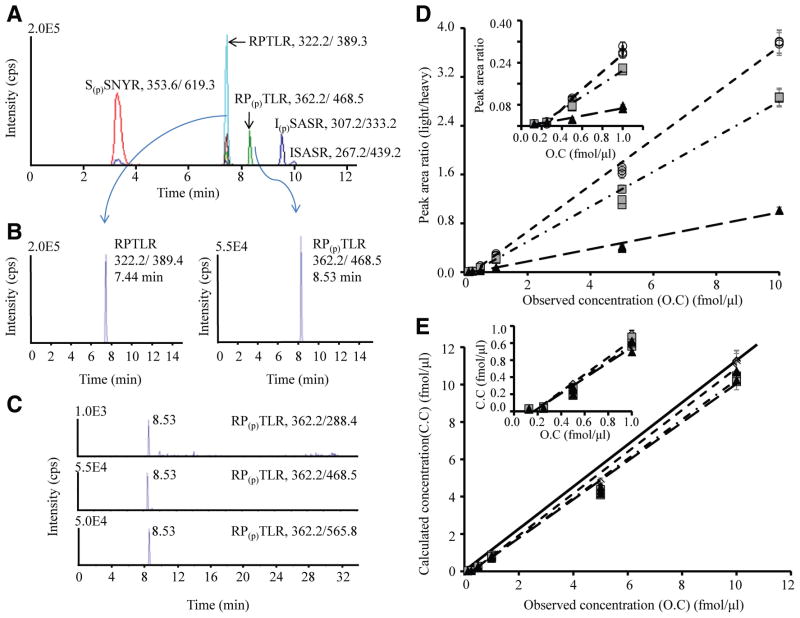
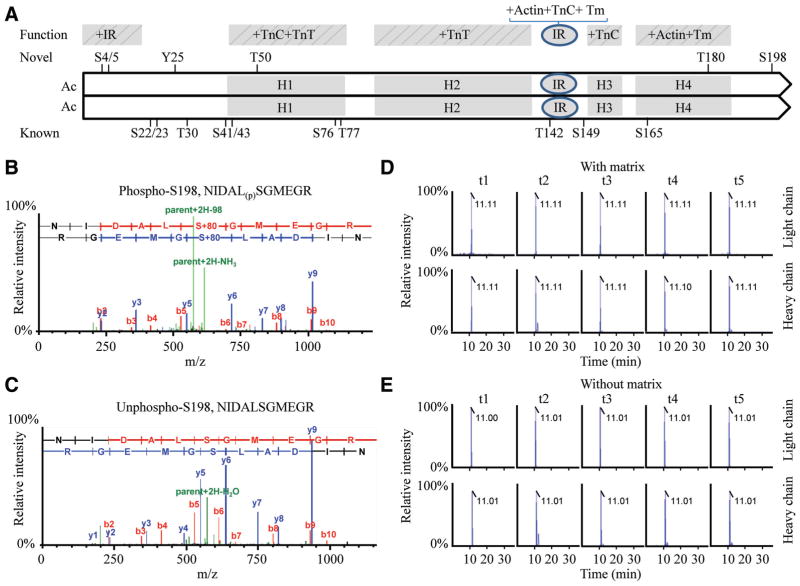
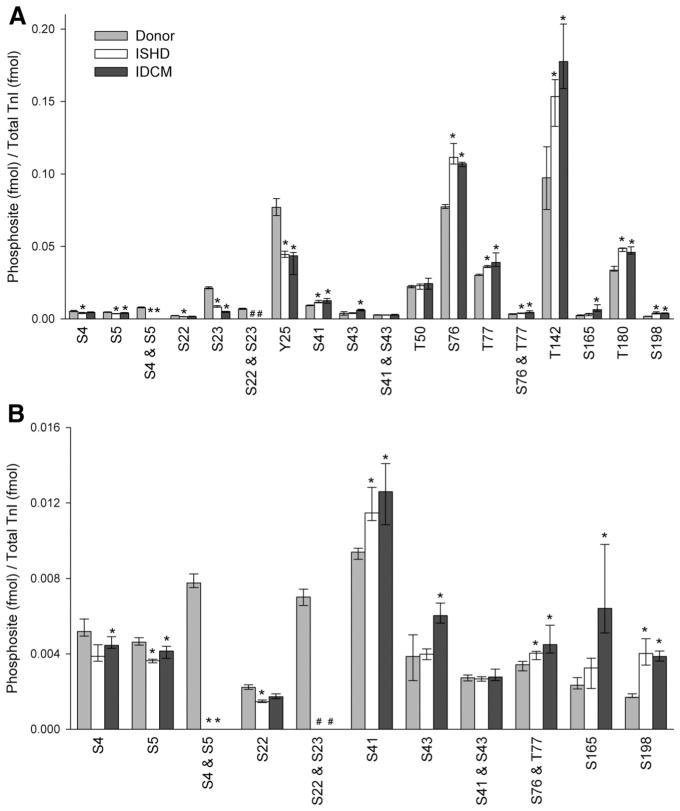
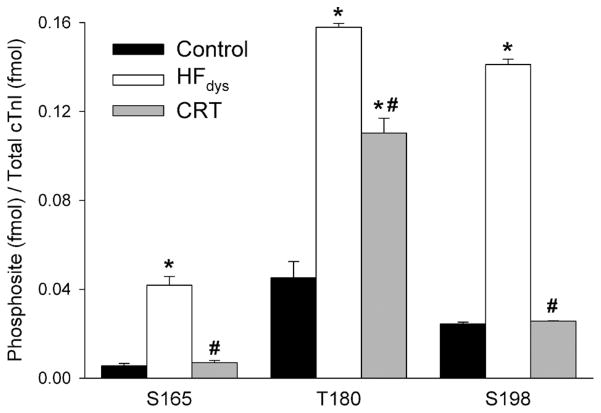
Methods and results: On the basis of in silico prediction and liquid chromatography/mass spectrometry data, 14 phosphorylation sites on cardiac troponin I, including 6 novel residues (S4, S5, Y25, T50, T180, S198), were assessed in explanted hearts from end-stage heart failure transplantation patients with ischemic heart disease or idiopathic dilated cardiomyopathy and compared with samples obtained from nonfailing donor hearts (n=10 per group). Thirty mass spectrometry-based multiple reaction monitoring quantitative tryptic peptide assays were developed for each phosphorylatable and corresponding nonphosphorylated site. The results show that in heart failure there is a decrease in the extent of phosphorylation of the known protein kinase A sites (S22, S23) and other newly discovered phosphorylation sites located in the N-terminal extension of cardiac troponin I (S4, S5, Y25), an increase in phosphorylation of the protein kinase C sites (S41, S43, T142), and an increase in phosphorylation of the IT-arm domain residues (S76, T77) and C-terminal domain novel phosphorylation sites of cardiac troponin I (S165, T180, S198). In a canine dyssynchronous heart failure model, enhanced phosphorylation at 3 novel sites was found to decline toward control after resynchronization therapy.
Conclusions: Selective, functionally significant phosphorylation alterations occurred on individual residues of cardiac troponin I in heart failure, likely reflecting an imbalance in kinase/phosphatase activity. Such changes can be reversed by cardiac resynchronization.
Figures
Comment in
-
Targeted proteomics for determining phosphorylation site-specific associations in cardiovascular disease.Circulation. 2012 Oct 9;126(15):1803-7. doi: 10.1161/CIRCULATIONAHA.112.136507. Epub 2012 Sep 12. Circulation. 2012. PMID: 22972901 No abstract available.
References
-
- Murphy AM. Heart failure, myocardial stunning, and troponin: a key regulator of the cardiac myofilament. Congest Heart Fail. 2006;12:32–38. - PubMed
-
- Zakhary DR, Moravec CS, Stewart RW, Bond M. Protein kinase A (PKA)-dependent troponin-I phosphorylation and PKA regulatory subunits are decreased in human dilated cardiomyopathy. Circulation. 1999;99:505–510. - PubMed
-
- Kobayashi T, Yang X, Walker LA, Van Breemen RB, Solaro RJ. A non-equilibrium isoelectric focusing method to determine states of phosphorylation of cardiac troponin I: identification of Ser-23 and Ser-24 as significant sites of phosphorylation by protein kinase C. J Mol Cell Cardiol. 2005;38:213–218. - PubMed
-
- Haworth RS, Cuello F, Herron TJ, Franzen G, Kentish JC, Gautel M, Avkiran M. Protein kinase D is a novel mediator of cardiac troponin I phosphorylation and regulates myofilament function. Circ Res. 2004;95:1091–1099. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
