

Gender differences in survival among adult patients starting antiretroviral therapy in South Africa: a multicentre cohort study
- PMID: 22973181
- PMCID: PMC3433409
- DOI: 10.1371/journal.pmed.1001304
Gender differences in survival among adult patients starting antiretroviral therapy in South Africa: a multicentre cohort study
Abstract
Background: Increased mortality among men on antiretroviral therapy (ART) has been documented but remains poorly understood. We examined the magnitude of and risk factors for gender differences in mortality on ART.
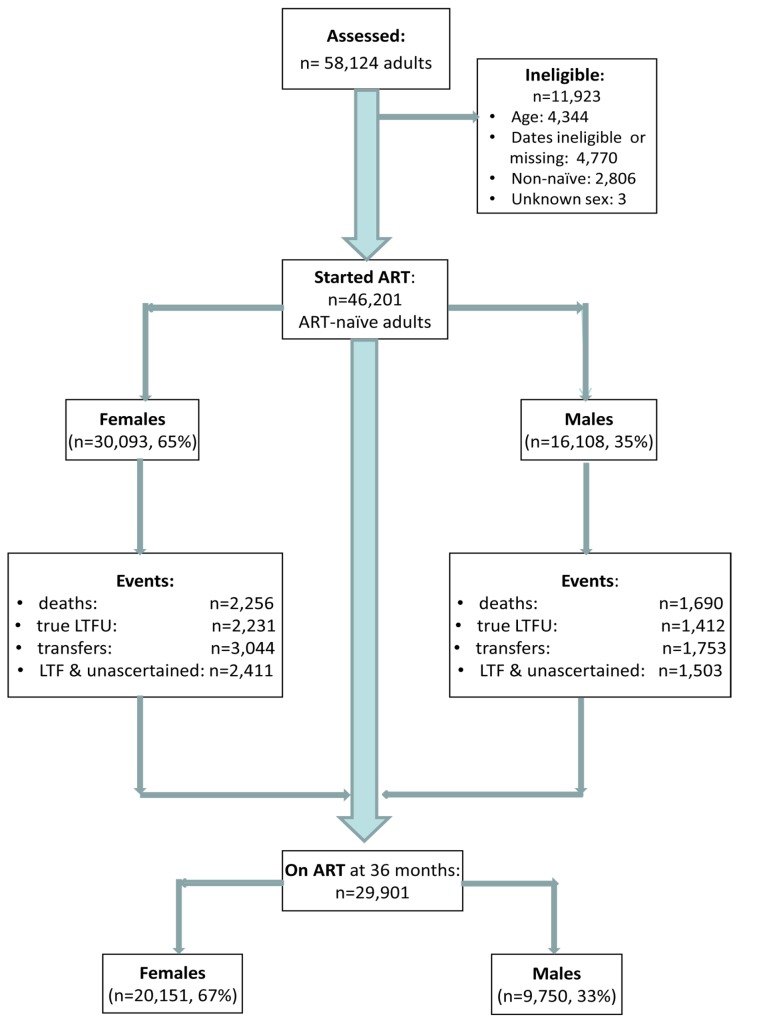
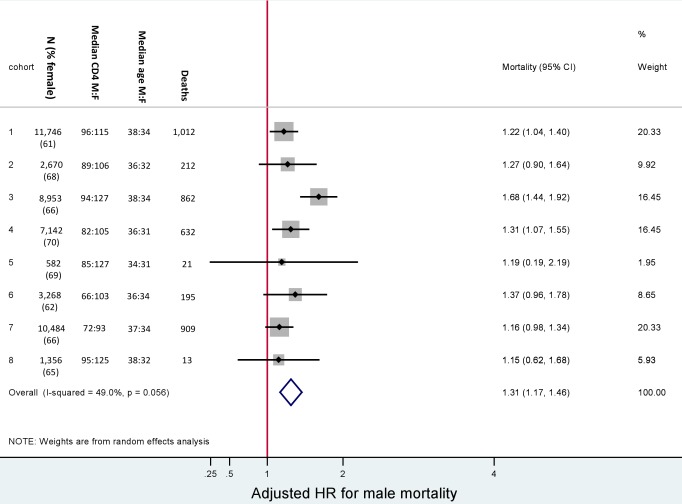
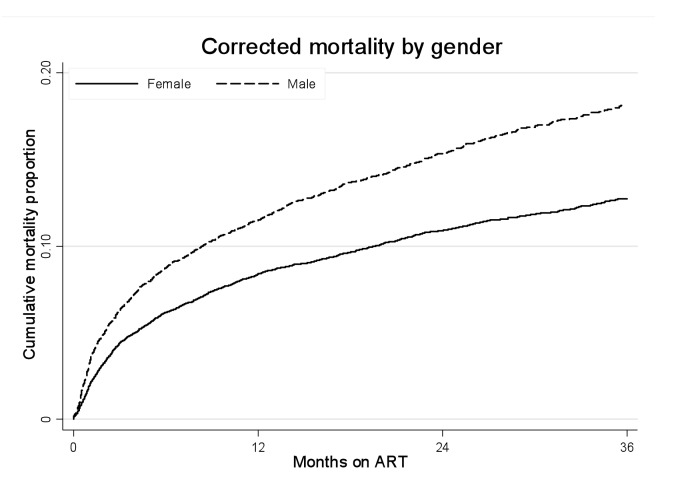
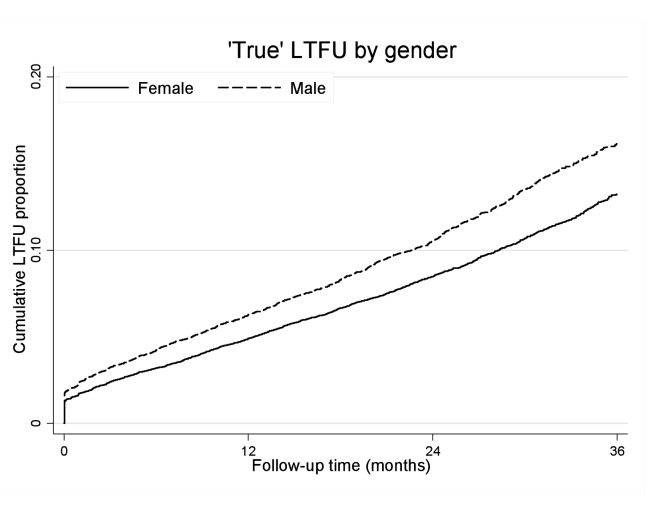
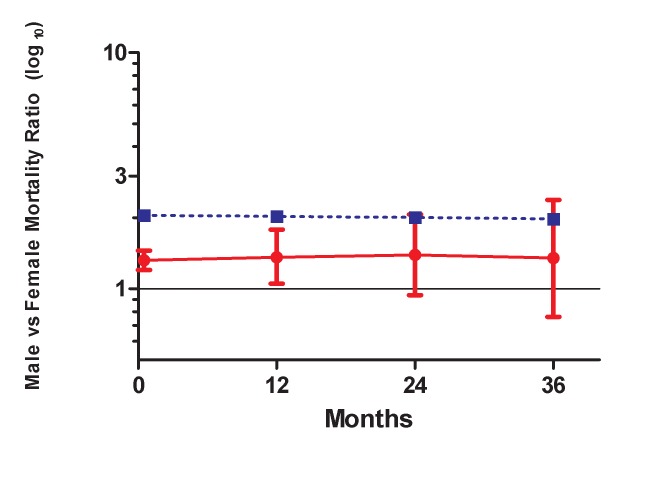
Methods and findings: Analyses included 46,201 ART-naïve adults starting ART between January 2002 and December 2009 in eight ART programmes across South Africa (SA). Patients were followed from initiation of ART to outcome or analysis closure. The primary outcome was mortality; secondary outcomes were loss to follow-up (LTF), virologic suppression, and CD4+ cell count responses. Survival analyses were used to examine the hazard of death on ART by gender. Sensitivity analyses were limited to patients who were virologically suppressed and patients whose CD4+ cell count reached >200 cells/µl. We compared gender differences in mortality among HIV+ patients on ART with mortality in an age-standardised HIV-negative population. Among 46,201 adults (65% female, median age 35 years), during 77,578 person-years of follow-up, men had lower median CD4+ cell counts than women (85 versus 110 cells/µl, p<0.001), were more likely to be classified WHO stage III/IV (86 versus 77%, p<0.001), and had higher mortality in crude (8.5 versus 5.7 deaths/100 person-years, p<0.001) and adjusted analyses (adjusted hazard ratio [AHR] 1.31, 95% CI 1.22-1.41). After 36 months on ART, men were more likely than women to be truly LTF (AHR 1.20, 95% CI 1.12-1.28) but not to die after LTF (AHR 1.04, 95% CI 0.86-1.25). Findings were consistent across all eight programmes. Virologic suppression was similar by gender; women had slightly better immunologic responses than men. Notably, the observed gender differences in mortality on ART were smaller than gender differences in age-standardised death rates in the HIV-negative South African population. Over time, non-HIV mortality appeared to account for an increasing proportion of observed mortality. The analysis was limited by missing data on baseline HIV disease characteristics, and we did not observe directly mortality in HIV-negative populations where the participating cohorts were located.
Conclusions: HIV-infected men have higher mortality on ART than women in South African programmes, but these differences are only partly explained by more advanced HIV disease at the time of ART initiation, differential LTF and subsequent mortality, and differences in responses to treatment. The observed differences in mortality on ART may be best explained by background differences in mortality between men and women in the South African population unrelated to the HIV/AIDS epidemic. Please see later in the article for the Editors' Summary.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Johnson L (2012) Access to antiretroviral treatment in South Africa, 2004–2011. S Afr J HIV Med 13: 22–27.
-
- Braitstein P, Boulle A, Nash D, Brinkhof M, Dabis F, et al. (2008) Gender and the use of antiretroviral treatment in resource-constrained settings: findings from a multicenter collaboration. J Womens Health (Larchmt) 17: 47–55. - PubMed
-
- Stenehjem E, Shlay JC (2008) Sex-specific differences in treatment outcomes for patients with HIV and AIDS. Expert Rev Pharmacoecon Outcomes Res 8: 51–63. - PubMed
-
- Hawkins C, Chalamilla G, Okuma J, Spiegelman D, Hertzmark E, et al. (2011) Gender differences in antiretroviral treatment outcomes among HIV-infected adults in Dar es Salaam, Tanzania. AIDS 25: 1189–1197. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
