

A comparison between early maternal and neonatal complications of restrictive episiotomy and routine episiotomy in primiparous vaginal delivery
- PMID: 22973367
- PMCID: PMC3434900
A comparison between early maternal and neonatal complications of restrictive episiotomy and routine episiotomy in primiparous vaginal delivery
Abstract
Background: Routine episiotomy is a controversial issue among gynecologists. The aim of this study was to compare early maternal and neonatal complications of restrictive episiotomy and routine episiotomy in primiparus vaginal delivery.
Methods: In this descriptive cross-sectional study, two groups of primiparus normal vaginal delivery (NVD) cases with routine and restrictive episiotomy were studied. Immediately and in the first 24 and 48 hours after delivery, specific charts were used to compare the two groups in terms of perineal laceration size, neonatal Apgar score and post-delivery. For data analysis, SPSS was used to conduct student t-test and Kruskal-Wallis test. A p-value < 0.05 was considered significant.
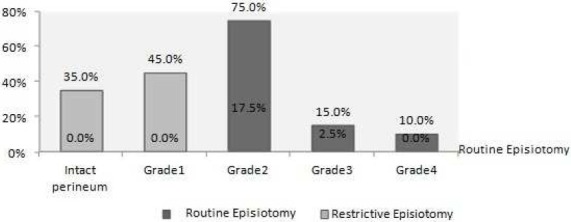
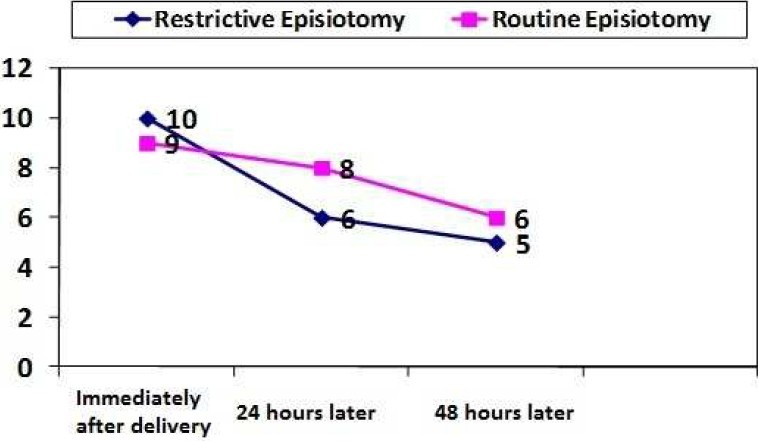
Results: Forty primiparus pregnant women were studied in each group. Episiotomy was performed in 7.5% of the restrictive group. Perineal laceration was measured as 3.68 ± 0.47 cm and 1.21 ± 1.1 in routine and restrictive episiotomy groups, respectively (p < 0.05). Intact perineum or first-degree laceration was seen in 80% of the restrictive group. However, second- and third-degree laceration were respectively observed in 75% and 15% of the routine episiotomy group (p < 0.05). Pain relief (immediately, 24 and 48 hours after delivery) was significantly higher in the restrictive group (p < 0.05). On the contrary, no significant difference in Apgar scores at the first and fifth minutes after birth was found between the two groups (p > 0.05).
Conclusions: Restrictive episiotomy results in low maternal complications. Therefore, avoiding routine episiotomy in unnecessary conditions would increase the rate of intact perineal and minor perineal trauma and reduce postpartum delivery pain with no adverse effects neither on maternal nor neonatal morbidities.
Keywords: Episiotomy; Normal Vaginal Delivery (NVD); Perineal Laceration.
Conflict of interest statement
Figures
References
-
- Weeks JD, Kozak LJ. Trends in the use of episiotomy in the United States: 1980-1998. Birth. 2001;28(3):152–60. - PubMed
-
- Kok J, Tan KH, Koh S, Cheng PS, Lim WY, Yew ML, et al. Antenatal use of a novel vaginal birth training device by term primiparous women in Singapore. Singapore Med J. 2004;45(7):318–23. - PubMed
-
- de Tayrac R, Panel L, Masson G, Mares P. Episiotomy and prevention of perineal and pelvic floor injuries. J Gynecol Obstet Biol Reprod (Paris) 2006;35(1 Suppl):1S24–31. [In French] - PubMed
-
- Hartmann K, Viswanathan M, Palmieri R, Gartlehner G, Thorp J, Jr, Lohr KN. Outcomes of routine episiotomy: a systematic review. JAMA. 2005;293(17):2141–8. - PubMed
LinkOut - more resources
Full Text Sources