

Substance abuse, HIV-1 and hepatitis
- PMID: 22973853
- PMCID: PMC3708479
- DOI: 10.2174/157016212803306023
Substance abuse, HIV-1 and hepatitis
Abstract
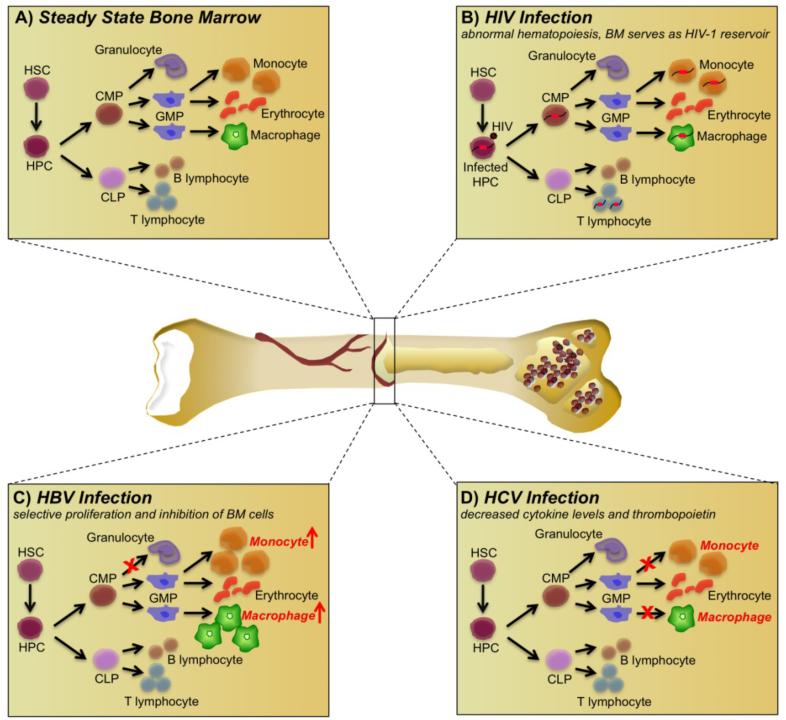
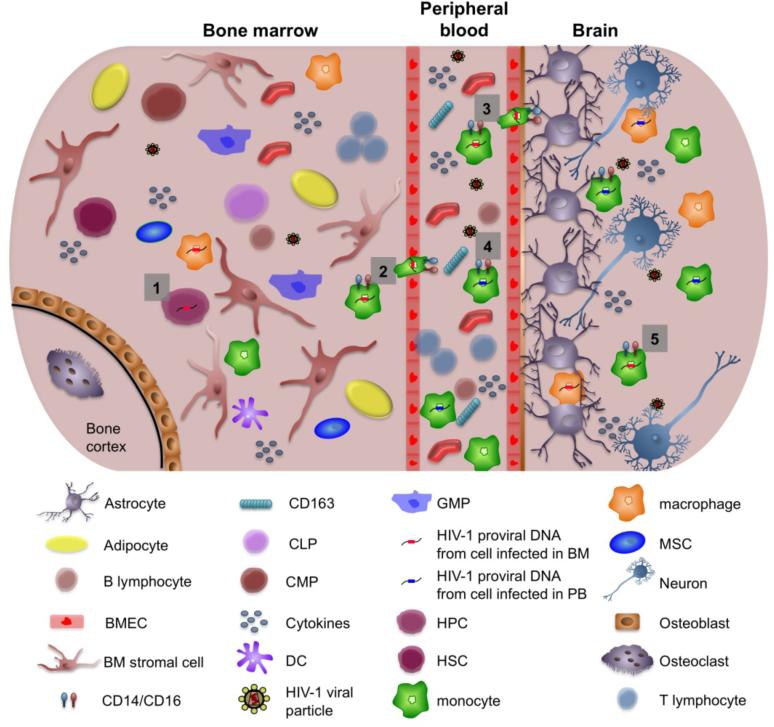
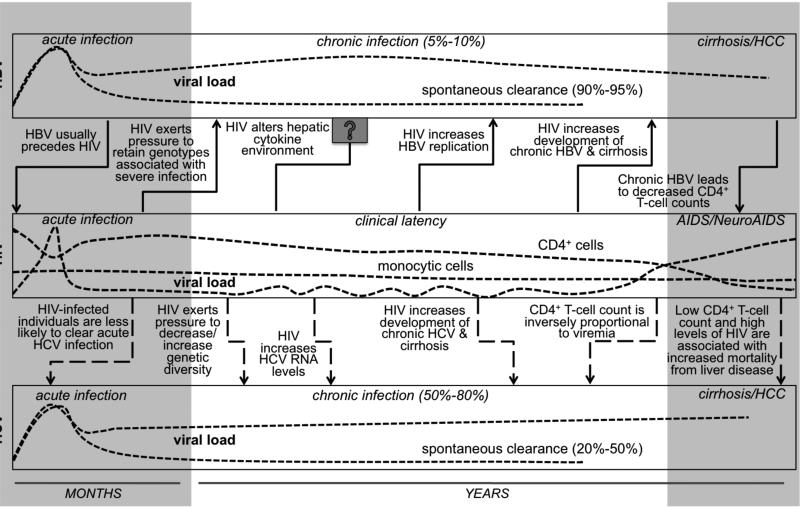
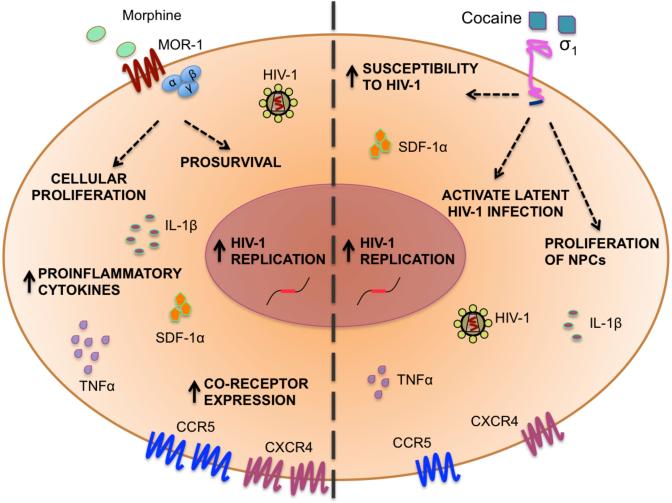
During the course of human immunodeficiency virus type 1 (HIV-1) disease, the virus has been shown to effectively escape the immune response with the subsequent establishment of latent viral reservoirs in specific cell populations within the peripheral blood (PB) and associated lymphoid tissues, bone marrow (BM), brain, and potentially other end organs. HIV-1, along with hepatitis B and C viruses (HBV and HCV), are known to share similar routes of transmission, including intravenous drug use, blood transfusions, sexual intercourse, and perinatal exposure. Substance abuse, including the use of opioids and cocaine, is a significant risk factor for exposure to HIV-1 and the development of acquired immune deficiency syndrome, as well as HBV and HCV exposure, infection, and disease. Thus, coinfection with HIV-1 and HBV or HCV is common and may be impacted by chronic substance abuse during the course of disease. HIV- 1 impacts the natural course of HBV and HCV infection by accelerating the progression of HBV/HCV-associated liver disease toward end-stage cirrhosis and quantitative depletion of the CD4+ T-cell compartment. HBV or HCV coinfection with HIV-1 is also associated with increased mortality when compared to either infection alone. This review focuses on the impact of substance abuse and coinfection with HBV and HCV in the PB, BM, and brain on the HIV-1 pathogenic process as it relates to viral pathogenesis, disease progression, and the associated immune response during the course of this complex interplay. The impact of HIV-1 and substance abuse on hepatitis virus-induced disease is also a focal point.
Figures
References
-
- 2010 Report on the global AIDS epidemic. UNAIDS/WHO; 2010.
-
- Bartlett JaFA. The Guide to Living with HIV Infection. Sixth ed A Johns Hopkins Press Health Book;
-
- Veazey RS, DeMaria M, Chalifoux LV, Shvetz DE, Pauley DR, Knight HL, et al. Gastrointestinal tract as a major site of CD4+ T cell depletion and viral replication in SIV infection. Science. 1998 Apr 17;280(5362):427–31. - PubMed
-
- Fierer DS, Klotman ME. Kidney and central nervous system as reservoirs of HIV infection. Curr Opin HIV AIDS. 2006 Mar;1(2):115–20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
