

Giant squamous cell carcinoma as a complication of a chronic enterocutaneous fistula: complex parietal reconstruction
- PMID: 22974076
- PMCID: PMC7950676
- DOI: 10.1111/j.1742-481X.2012.01088.x
Giant squamous cell carcinoma as a complication of a chronic enterocutaneous fistula: complex parietal reconstruction
Abstract
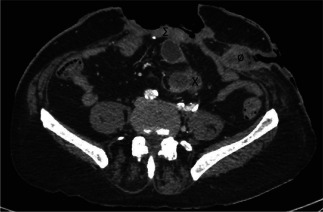
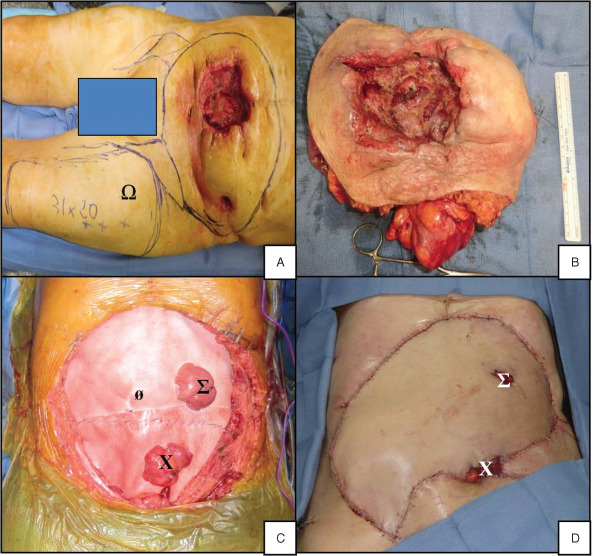
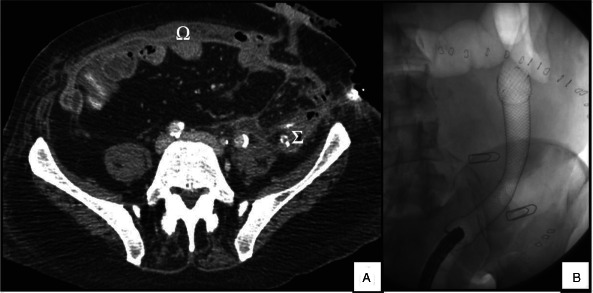
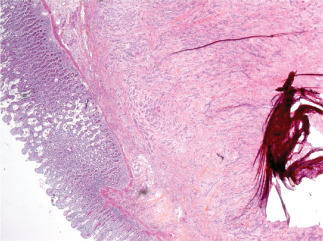
Treatment of an enterocutaneous fistula is complex and may require multidisciplinary management, especially when associated with a neoplastic process. Here, we describe the case of a 59-year-old patient with a squamous cell carcinoma that had invaded the abdominal wall through a chronic enterocutaneous fistula identified 30 years ago. We combined parietectomy with small intestine and colon resection and inguinal lymphadenectomy in order to obtain clear surgical margins. At the same time, plastic surgery involved the implementation of a large bioprosthesis and coverage with a vastus lateralis muscle free flap.
Keywords: Abdominal parietectomy; Bioprosthesis; Parietal squamous cell carcinoma.
© 2012 The Authors. International Wound Journal © 2012 Medicalhelplines.com Inc and John Wiley & Sons Ltd.
Figures

Similar articles
-
Abdominal wall reconstruction after resection of an enterocutaneous fistula with an island pedicled anterolateral thigh perforator flap. Case report.Clin Ter. 2013;164(5):413-5. doi: 10.7417/CT.2013.1605. Clin Ter. 2013. PMID: 24217827
-
[Crohn's disease complicated with squamous cell carcinoma originating from an enterocutaneous fistula:a case report].Nihon Shokakibyo Gakkai Zasshi. 2025;122(1):51-58. doi: 10.11405/nisshoshi.122.51. Nihon Shokakibyo Gakkai Zasshi. 2025. PMID: 39805623 Japanese.
-
Complex abdominal wall reconstruction after radiation therapy: a full-thickness defect was repaired with a rectus femoris myofasciocutaneous flap.Am J Obstet Gynecol. 2009 Jan;200(1):116.e1-3. doi: 10.1016/j.ajog.2008.10.004. Am J Obstet Gynecol. 2009. PMID: 19121665 No abstract available.
-
Takedown of enterocutaneous fistula and complex abdominal wall reconstruction.Surg Clin North Am. 2013 Oct;93(5):1163-83. doi: 10.1016/j.suc.2013.06.006. Epub 2013 Jul 26. Surg Clin North Am. 2013. PMID: 24035080 Review.
-
Use of human and porcine dermal-derived bioprostheses in complex abdominal wall reconstructions: a literature review and case report.Ostomy Wound Manage. 2007 May;53(5):30-7. Ostomy Wound Manage. 2007. PMID: 17551173 Review.
References
-
- Draus JMJr, Huss SA, Harty NJ, Cheadle WG, Larson GM. Enterocutaneous fistula: are treatments improving? Surgery 2006;140:570–6. - PubMed
-
- Tassiopoulos AK, Baum G, Halverson JD. Small bowel fistulas. Surg Clin North Am 1996;76:1175–81. - PubMed
-
- Lloyd DA, Gabe SM, Windsor AC. Nutrition and management of enterocutaneous fistula. Br J Surg 2006;93:1045–55. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
