

Racial disparity in fracture risk between white and nonwhite children in the United States
- PMID: 22974572
- PMCID: PMC3504618
- DOI: 10.1016/j.jpeds.2012.07.054
Racial disparity in fracture risk between white and nonwhite children in the United States
Abstract
Objectives: To examine risk factors for fracture in a racially diverse cohort of healthy children in the US.
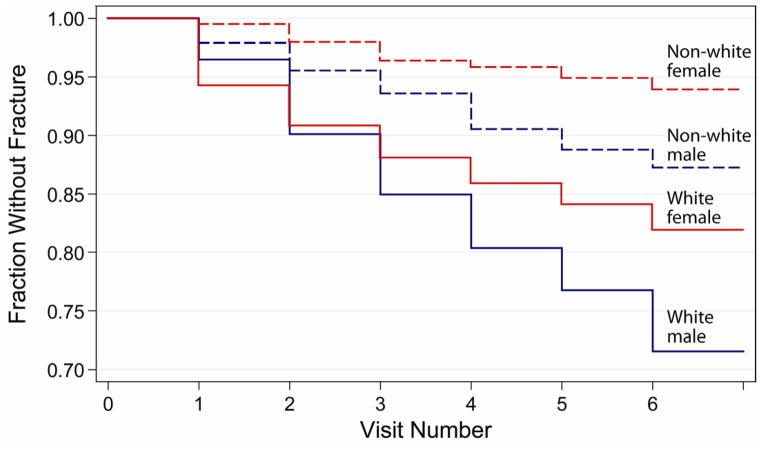
Study design: A total of 1470 healthy children, aged 6-17 years, underwent yearly evaluations of height, weight, body mass index, skeletal age, sexual maturation, calcium intake, physical activity levels, and dual-energy x-ray absorptiometry (DXA) bone and fat measurements for up to 6 years. Fracture information was obtained at each annual visit, and risk factors for fracture were examined using the time-dependent Cox proportional hazards model.
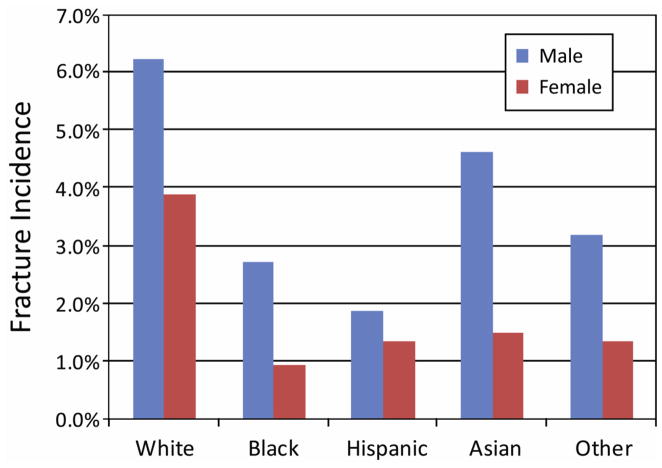
Results: The overall fracture incidence was 0.034 fracture per person-year with 212 children reporting a total of 257 fractures. Being white (hazard ratio [HR] = 2.1), being male (HR = 1.8), and having skeletal age of 10-14 years (HR = 2.2) were the strongest risk factors for fracture (all P ≤ .001). Increased sports participation (HR = 1.4), lower body fat percentage (HR = 0.97), and previous fracture in white girls (HR = 2.1) were also significant risk factors (all P ≤ .04). Overall, fracture risk decreased with higher DXA z scores, except in white boys, who had increased fracture risk with higher DXA z scores (HR = 1.7, P < .001).
Conclusions: Boys and girls of European descent had double the fracture risk of children from other backgrounds, suggesting that the genetic predisposition to fractures seen in elderly adults also manifests in children.
Copyright © 2012 Mosby, Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- N01-HD-1-3331/HD/NICHD NIH HHS/United States
- N01 HD013329/HD/NICHD NIH HHS/United States
- N01-HD-1-3332/HD/NICHD NIH HHS/United States
- N01 HD013331/HD/NICHD NIH HHS/United States
- N01 HD013328/HD/NICHD NIH HHS/United States
- N01-HD-1-3329/HD/NICHD NIH HHS/United States
- UL1 TR000077/TR/NCATS NIH HHS/United States
- N01 HD013333/HD/NICHD NIH HHS/United States
- N01 HD013330/HD/NICHD NIH HHS/United States
- N01-HD-1-3228/HD/NICHD NIH HHS/United States
- N01-HD-1-3330/HD/NICHD NIH HHS/United States
- N01-HD-1-3333/HD/NICHD NIH HHS/United States
- N01 HD013332/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
