

Comparative effectiveness of 5 treatment strategies for early-stage non-small cell lung cancer in the elderly
- PMID: 22975611
- PMCID: PMC3776428
- DOI: 10.1016/j.ijrobp.2012.07.2354
Comparative effectiveness of 5 treatment strategies for early-stage non-small cell lung cancer in the elderly
Abstract
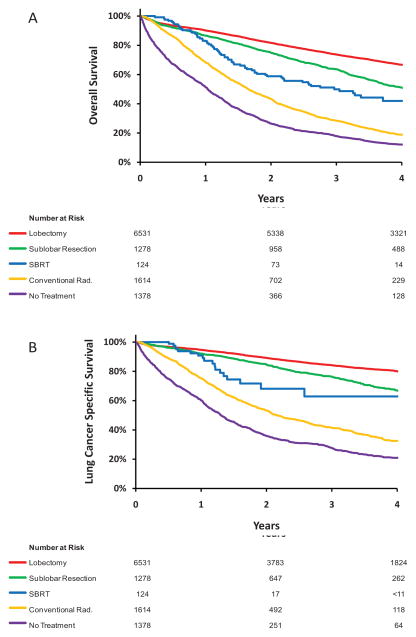
Purpose: The incidence of early-stage non-small cell lung cancer (NSCLC) among older adults is expected to increase because of demographic trends and computed tomography-based screening; yet, optimal treatment in the elderly remains controversial. Using the Surveillance, Epidemiology, and End Results (SEER)-Medicare cohort spanning 2001-2007, we compared survival outcomes associated with 5 strategies used in contemporary practice: lobectomy, sublobar resection, conventional radiation therapy, stereotactic ablative radiation therapy (SABR), and observation.
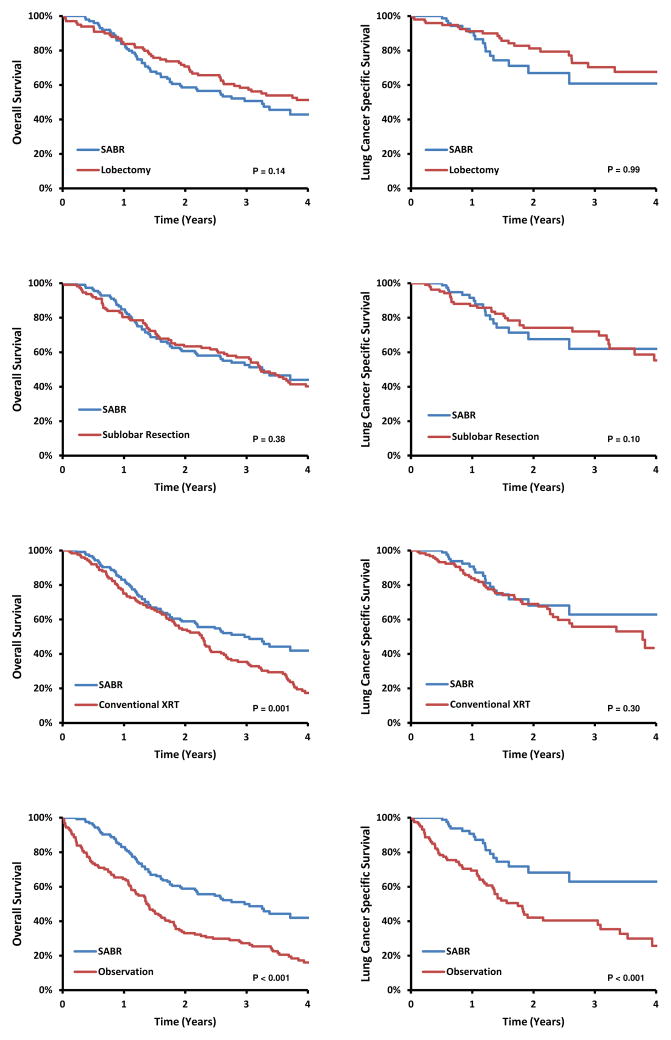
Methods and materials: Treatment strategy and covariates were determined in 10,923 patients aged ≥ 66 years with stage IA-IB NSCLC. Cox regression, adjusted for patient and tumor factors, compared overall and disease-specific survival for the 5 strategies. In a second exploratory analysis, propensity-score matching was used for comparison of SABR with other options.
Results: The median age was 75 years, and 29% had moderate to severe comorbidities. Treatment distribution was lobectomy (59%), sublobar resection (11.7%), conventional radiation (14.8%), observation (12.6%), and SABR (1.1%). In Cox regression analysis with a median follow-up time of 3.2 years, SABR was associated with the lowest risk of death within 6 months of diagnosis (hazard ratio [HR] 0.48; 95% confidence interval [CI] 0.38-0.63; referent is lobectomy). After 6 months, lobectomy was associated with the best overall and disease-specific survival. In the propensity-score matched analysis, survival after SABR was similar to that after lobectomy (HR 0.71; 95% CI 0.45-1.12; referent is SABR). Conventional radiation and observation were associated with poor outcomes in all analyses.
Conclusions: In this population-based experience, lobectomy was associated with the best long-term outcomes in fit elderly patients with early-stage NSCLC. Exploratory analysis of SABR early adopters suggests efficacy comparable with that of surgery in select populations. Evaluation of these therapies in randomized trials is urgently needed.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Early-stage non-small cell lung cancer in elderly patients: should stereotactic radiation therapy be the standard of care?Int J Radiat Oncol Biol Phys. 2012 Dec 1;84(5):1058-9. doi: 10.1016/j.ijrobp.2012.07.2353. Int J Radiat Oncol Biol Phys. 2012. PMID: 23140576 No abstract available.
References
-
- Rami-Porta R, Crowley JJ, Goldstraw P. The revised TNM staging system for lung cancer. Ann Thorac Cardiovasc Surg. 2009;15:4–9. - PubMed
-
- Smith BD, Smith GL, Hurria A, et al. Future of cancer incidence in the United States: burdens upon an aging, changing nation. J Clin Oncol. 2009;27:2758–2765. - PubMed
-
- Warren JL, Klabunde CN, Schrag D, et al. Overview of the SEER-Medicare data: content, research applications, and generalizability to the United States elderly population. Med Care. 2002;40:IV-3–18. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
