

Serum proteins reflecting inflammation, injury and repair as biomarkers of disease activity in ANCA-associated vasculitis
- PMID: 22975753
- PMCID: PMC4982463
- DOI: 10.1136/annrheumdis-2012-201981
Serum proteins reflecting inflammation, injury and repair as biomarkers of disease activity in ANCA-associated vasculitis
Abstract
Objective: To identify circulating proteins that distinguish between active anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) and remission in a manner complementary to markers of systemic inflammation.
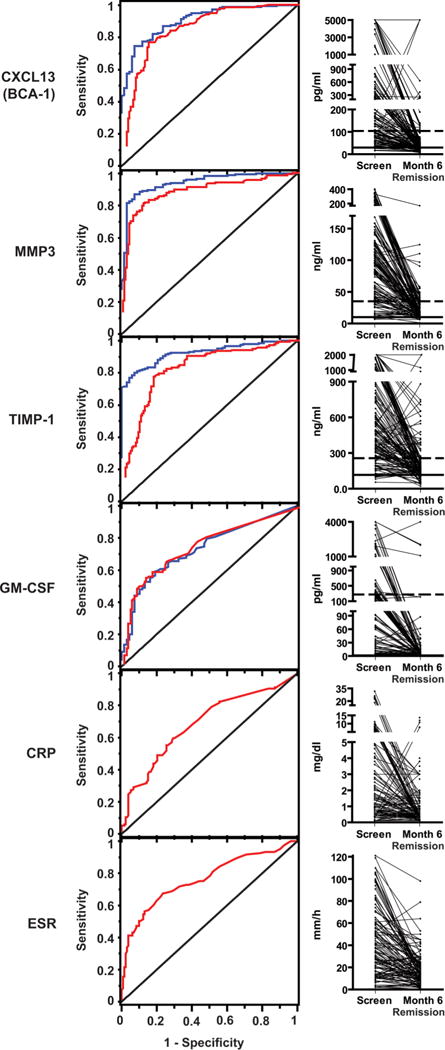
Methods: Twenty-eight serum proteins representing diverse aspects of the biology of AAV were measured before and 6 months after treatment in a large clinical trial of AAV. Subjects (n=186) enrolled in the Rituximab in ANCA-Associated Vasculitis (RAVE) trial were studied. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels were available for comparison. The primary outcome was the ability of markers to distinguish severe AAV (Birmingham Vasculitis Activity Score for Wegener's granulomatosis (BVAS/WG)≥3 at screening) from remission (BVAS/WG=0 at month 6), using areas under receiver operating characteristic (ROC) curve (AUC).
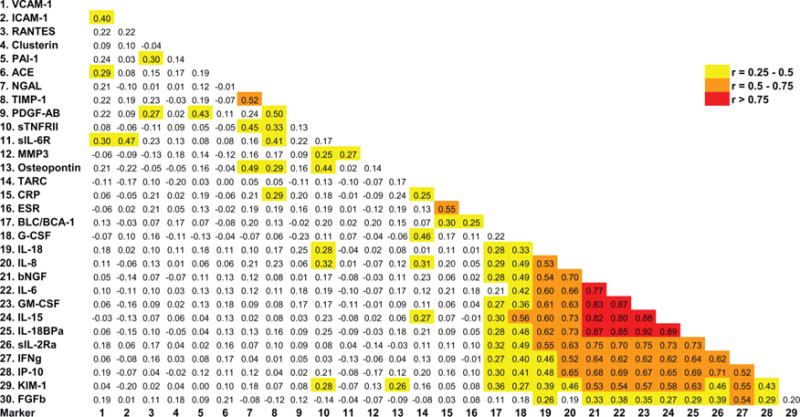
Results: All subjects had severe active vasculitis (median BVAS/WG=8) at screening. In the 137 subjects in remission at month 6, 24 of the 28 markers showed significant declines. ROC analysis indicated that levels of CXCL13 (BCA-1), matrix metalloproteinase-3 (MMP-3) and tissue inhibitor of metalloproteinases-1 (TIMP-1) best discriminated active AAV from remission (AUC>0.8) and from healthy controls (AUC>0.9). Correlations among these markers and with ESR or CRP were low.
Conclusions: Many markers are elevated in severe active AAV and decline with treatment, but CXCL13, MMP-3 and TIMP-1 distinguish active AAV from remission better than the other markers studied, including ESR and CRP. These proteins are particularly promising candidates for future studies to address unmet needs in the assessment of patients with AAV.
Keywords: Autoimmune Diseases; Chemokines; Cytokines.
Conflict of interest statement
Figures
References
-
- Kerr GS, Fleisher TA, Hallahan CW, et al. Limited prognostic value of changes in antineutrophil cytoplasmic antibody titer in patients with Wegener’s granulomatosis. Arthritis Rheum. 1993;36:365–71. - PubMed
-
- Kyndt X, Reumaux D, Bridoux F, et al. Serial measurements of antineutrophil cytoplasmic autoantibodies in patients with systemic vasculitis. Am J Med. 1999;106:527–33. - PubMed
-
- Boomsma MM, Stegeman CA, van der Leij MJ, et al. Prediction of relapses in Wegener’s granulomatosis by measurement of antineutrophil cytoplasmic antibody levels: a prospective study. Arthritis Rheum. 2000;43:2025–33. - PubMed
-
- Girard T, Mahr A, Noel LH, et al. Are antineutrophil cytoplasmic antibodies a marker predictive of relapse in Wegener’s granulomatosis? A prospective study. Rheumatology (Oxford) 2001;40:147–51. - PubMed
-
- Finkielman JD, Merkel PA, Schroeder D, et al. Antiproteinase 3 antineutrophil cytoplasmic antibodies and disease activity in Wegener granulomatosis. Ann Intern Med. 2007;147:611–19. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- RR024150-01/RR/NCRR NIH HHS/United States
- K24 AR02224/AR/NIAMS NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- K23 AR052820/AR/NIAMS NIH HHS/United States
- M01 RR000533/RR/NCRR NIH HHS/United States
- UL1 RR025771/RR/NCRR NIH HHS/United States
- P60 AR047785/AR/NIAMS NIH HHS/United States
- U54 RR019497/RR/NCRR NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 RR024150/RR/NCRR NIH HHS/United States
- U54AR057319/AR/NIAMS NIH HHS/United States
- RC1 AR058303/AR/NIAMS NIH HHS/United States
- N01 AI015416/AI/NIAID NIH HHS/United States
- K24 AR002224/AR/NIAMS NIH HHS/United States
- NS064808/NS/NINDS NIH HHS/United States
- RR 025771/RR/NCRR NIH HHS/United States
- U54 NS064808/NS/NINDS NIH HHS/United States
- M01 RR00533/RR/NCRR NIH HHS/United States
- K24 AR049185/AR/NIAMS NIH HHS/United States
- RR025005/RR/NCRR NIH HHS/United States
- U54 AR057319/AR/NIAMS NIH HHS/United States
- P60AR047785/AR/NIAMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
