

A simple decision analytic solution to the comparison of two binary diagnostic tests
- PMID: 22975863
- PMCID: PMC3531575
- DOI: 10.1002/sim.5601
A simple decision analytic solution to the comparison of two binary diagnostic tests
Abstract
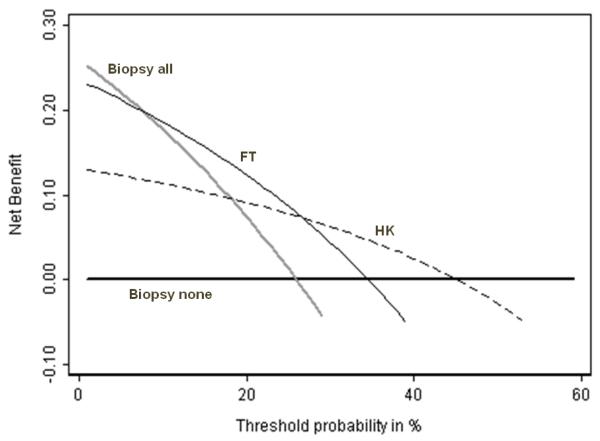
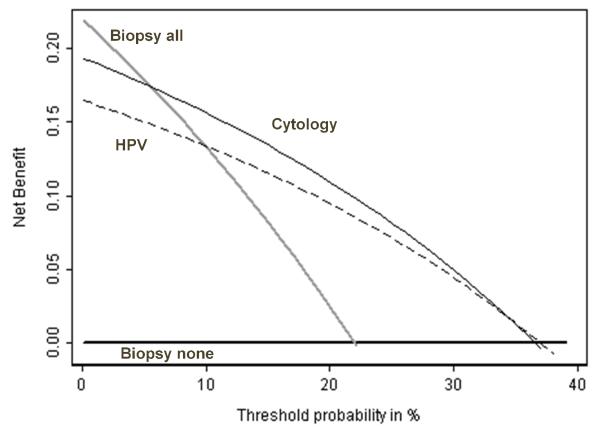
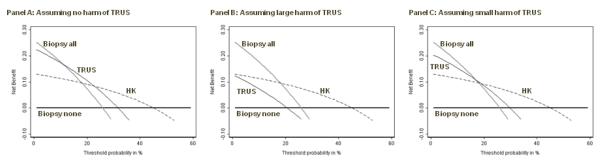
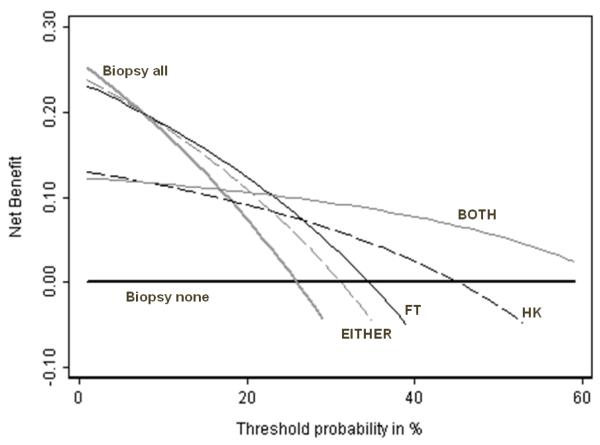
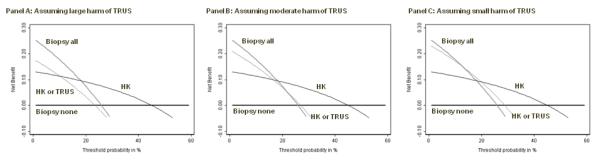
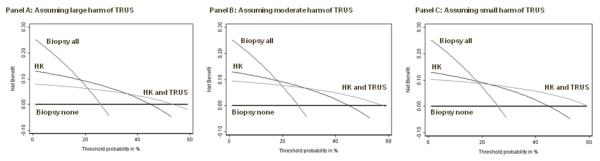
One of the most basic biostatistical problems is the comparison of two binary diagnostic tests. Commonly, one test will have greater sensitivity, and the other greater specificity. In this case, the choice of the optimal test generally requires a qualitative judgment as to whether gains in sensitivity are offset by losses in specificity. Here, we propose a simple decision analytic solution in which sensitivity and specificity are weighted by an intuitive parameter, the threshold probability of disease at which a patient will opt for treatment. This gives a net benefit that can be used to determine which of two diagnostic tests will give better clinical results at a given threshold probability and whether either is superior to the strategy of assuming that all or no patients have disease. We derive a simple formula for the relative diagnostic value, which is the difference in sensitivities of two tests divided by the difference in the specificities. We show that multiplying relative diagnostic value by the odds at the prevalence gives the odds of the threshold probability below which the more sensitive test is preferable and above which the more specific test should be chosen. The methodology is easily extended to incorporate combinations of tests and the risk or side effects of a test.
Copyright © 2012 John Wiley & Sons, Ltd.
Figures
Comment in
-
Remarks on 'A simple decision analytic solution to the comparison of two binary diagnostic tests' by Vickers et al.Stat Med. 2013 Feb 20;32(4):718. doi: 10.1002/sim.5663. Stat Med. 2013. PMID: 23341085 Free PMC article. No abstract available.
References
-
- Biggerstaff BJ. Comparing diagnostic tests: a simple graphic using likelihood ratios. Stat Med. 2000;19:649–663. DOI 10.1002/(SICI)1097-0258(20000315)19:5. - PubMed
-
- Macaskill P, Walter SD, Irwig L, Franco EL. Assessing the gain in diagnostic performance when combining two diagnostic tests. Stat Med. 2002;21:2527–2546. DOI 10.1002/sim.1227. - PubMed
-
- Bennett BM. On comparisons of sensitivity, specificity and predictive value of a number of diagnostic procedures. Biometrics. 1972;28:793–800. - PubMed
-
- Nofuentes JA, Del Castillo Jde D. Comparison of the likelihood ratios of two binary diagnostic tests in paired designs. Stat Med. 2007;26:4179–4201. DOI 10.1002/sim.2850 [doi] - PubMed
-
- Lu Y, Jin H, Genant HK. On the non-inferiority of a diagnostic test based on paired observations. Stat Med. 2003;22:3029–3044. DOI 10.1002/sim.1569. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical