

Association of mild to moderate chronic kidney disease with venous thromboembolism: pooled analysis of five prospective general population cohorts
- PMID: 22977129
- PMCID: PMC3520022
- DOI: 10.1161/CIRCULATIONAHA.112.113944
Association of mild to moderate chronic kidney disease with venous thromboembolism: pooled analysis of five prospective general population cohorts
Abstract
Background: Recent findings suggest that chronic kidney disease (CKD) may be associated with an increased risk of venous thromboembolism (VTE). Given the high prevalence of mild-to-moderate CKD in the general population, in depth analysis of this association is warranted.
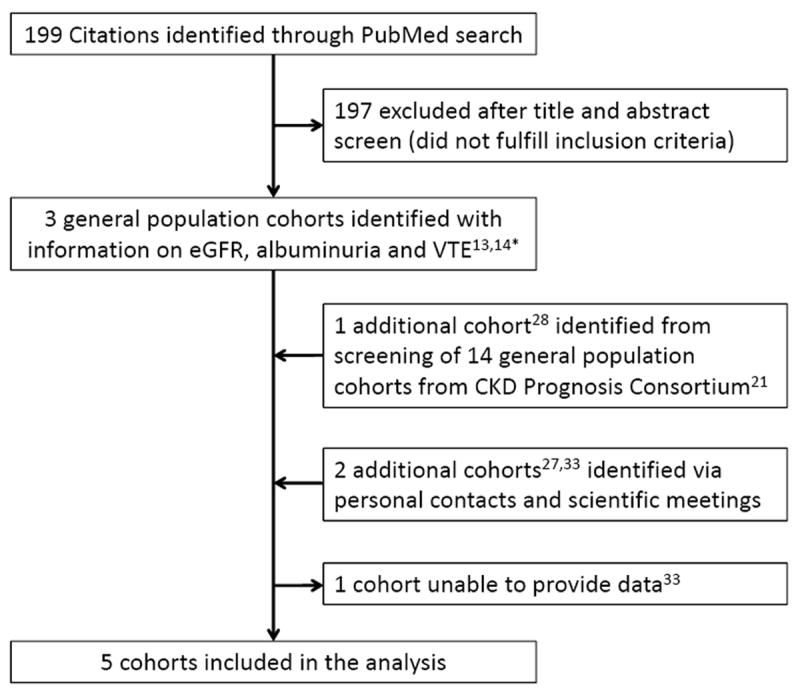
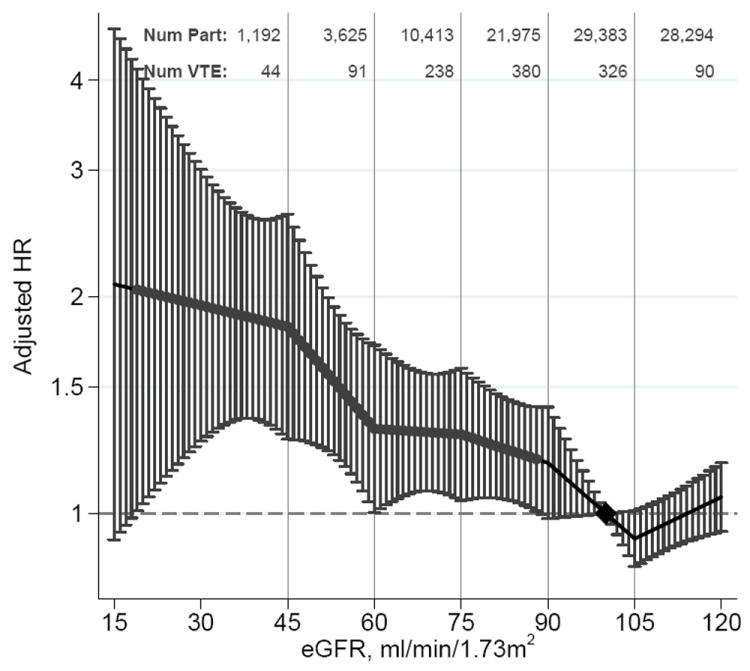
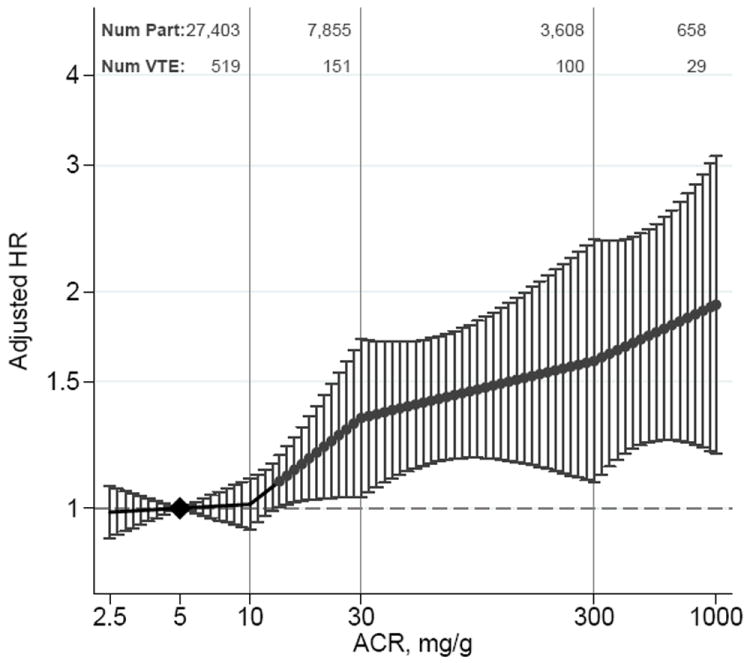
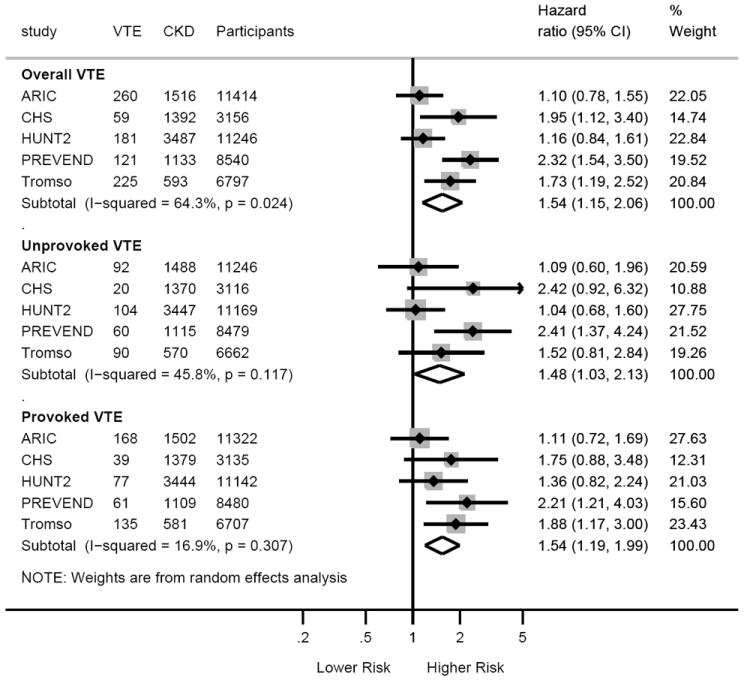
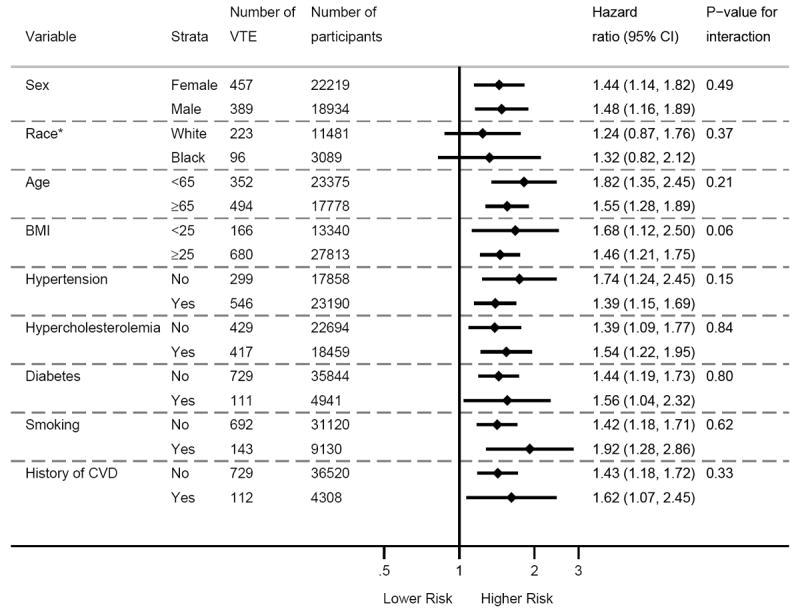
Methods and results: We pooled individual participant data from 5 community-based cohorts from Europe (second Nord-Trøndelag Health Study [HUNT2], Prevention of Renal and Vascular End-stage Disease [PREVEND], and the Tromsø study) and the United States (Atherosclerosis Risks in Communities [ARIC] and Cardiovascular Health Study [CHS]) to assess the association of estimated glomerular filtration rate (eGFR), albuminuria, and CKD with objectively verified VTE. To estimate adjusted hazard ratios for VTE, categorical and continuous spline models were fit by using Cox regression with shared-frailty or random-effect meta-analysis. A total of 1178 VTE events occurred over 599 453 person-years follow-up. Relative to eGFR 100 mL/min per 1.73 m(2), hazard ratios for VTE were 1.29 (95% confidence interval, 1.04-1.59) for eGFR 75, 1.31 (1.00-1.71) for eGFR 60, 1.82 (1.27-2.60) for eGFR 45, and 1.95 (1.26-3.01) for eGFR 30 mL/min per 1.73 m(2). In comparison with an albumin-to-creatinine ratio (ACR) of 5.0 mg/g, the hazard ratios for VTE were 1.34 (1.04-1.72) for ACR 30 mg/g, 1.60 (1.08-2.36) for ACR 300 mg/g, and 1.92 (1.19-3.09) for ACR 1000 mg/g. There was no interaction between clinical categories of eGFR and ACR (P=0.20). The adjusted hazard ratio for CKD, defined as eGFR <60 mL/min per 1.73 m(2) or albuminuria ≥30 mg/g, (versus no CKD) was 1.54 (95% confidence interval, 1.15-2.06). Associations were consistent in subgroups according to age, sex, and comorbidities, and for unprovoked versus provoked VTE, as well.
Conclusions: Both eGFR and ACR are independently associated with increased risk of VTE in the general population, even across the normal eGFR and ACR ranges.
Conflict of interest statement
Figures
Comment in
-
Venous thromboembolism: yet another cardiovascular complication of chronic kidney disease?Circulation. 2012 Oct 16;126(16):1937-8. doi: 10.1161/CIRCULATIONAHA.112.138057. Circulation. 2012. PMID: 23071175 No abstract available.
References
-
- Naess IA, Christiansen SC, Romundstad P, Cannegieter SC, Rosendaal FR, Hammerstrom J. Incidence and mortality of venous thrombosis: A population-based study. J Thromb Haemost. 2007;5:692–699. - PubMed
-
- Nordstrom M, Lindblad B, Bergqvist D, Kjellstrom T. A prospective study of the incidence of deep-vein thrombosis within a defined urban population. J Intern Med. 1992;232:155–160. - PubMed
-
- White RH. The epidemiology of venous thromboembolism. Circulation. 2003;107:I4–8. - PubMed
-
- Cushman M, Tsai AW, White RH, Heckbert SR, Rosamond WD, Enright P, Folsom AR. Deep vein thrombosis and pulmonary embolism in two cohorts: The Longitudinal Investigation of Thromboembolism Etiology. Am J Med. 2004;117:19–25. - PubMed
-
- Mahmoodi BK, ten Kate MK, Waanders F, Veeger NJ, Brouwer JL, Vogt L, Navis G, van der Meer J. High absolute risks and predictors of venous and arterial thromboembolic events in patients with nephrotic syndrome: Results from a large retrospective cohort study. Circulation. 2008;117:224–230. - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- R01 HL059367/HL/NHLBI NIH HHS/United States
- AG-20098/AG/NIA NIH HHS/United States
- N01-HC-85086/HC/NHLBI NIH HHS/United States
- AG-027058/AG/NIA NIH HHS/United States
- N01-HC-75150/HC/NHLBI NIH HHS/United States
- R01 HL080295/HL/NHLBI NIH HHS/United States
- HL080295/HL/NHLBI NIH HHS/United States
- N01 HC085081/HC/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- N01 CN015103/CA/NCI NIH HHS/United States
- R01 AG015928/AG/NIA NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- N01 HC075150/HC/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- N01 HC015103/HC/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HC/NHLBI NIH HHS/United States
- R56 AG020098/AG/NIA NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- R01 HL59367/HL/NHLBI NIH HHS/United States
- N01 HC085085/HC/NHLBI NIH HHS/United States
- N01 HC085082/HC/NHLBI NIH HHS/United States
- HL59367/HL/NHLBI NIH HHS/United States
- N01 HC085080/HC/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- N01 HC-55222/HC/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- N01 HC055222/HC/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- N01 HC085084/HC/NHLBI NIH HHS/United States
- R01 AG020098/AG/NIA NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- N01-HC-85079/HC/NHLBI NIH HHS/United States
- N01-HC-85239/HC/NHLBI NIH HHS/United States
- AG-023629/AG/NIA NIH HHS/United States
- N01 HC085079/HC/NHLBI NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- R01 AG027058/AG/NIA NIH HHS/United States
- N01 HC045133/HC/NHLBI NIH HHS/United States
- N01 HC035129/HC/NHLBI NIH HHS/United States
- R56 AG023629/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
