

Influence of common genetic variation on blood lipid levels, cardiovascular risk, and coronary events in two British prospective cohort studies
- PMID: 22977227
- PMCID: PMC3612774
- DOI: 10.1093/eurheartj/ehs243
Influence of common genetic variation on blood lipid levels, cardiovascular risk, and coronary events in two British prospective cohort studies
Abstract
Aims: The aim of this study was to quantify the collective effect of common lipid-associated single nucleotide polymorphisms (SNPs) on blood lipid levels, cardiovascular risk, use of lipid-lowering medication, and risk of coronary heart disease (CHD) events.
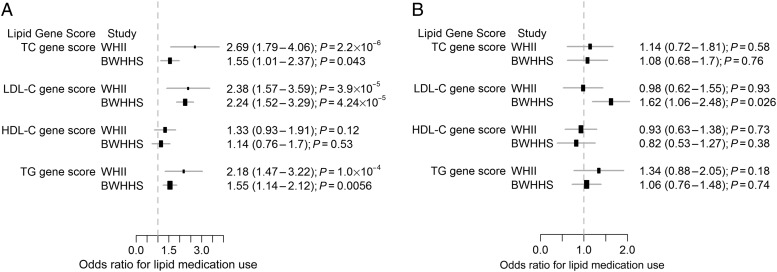
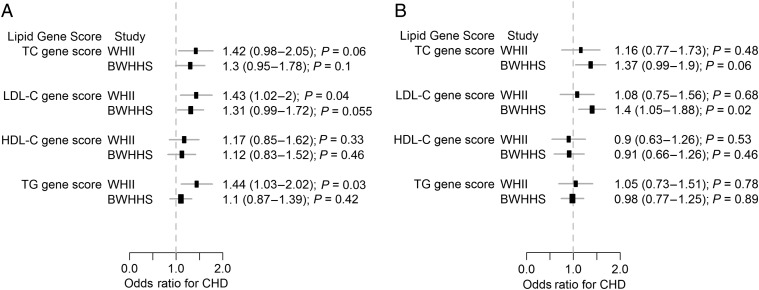
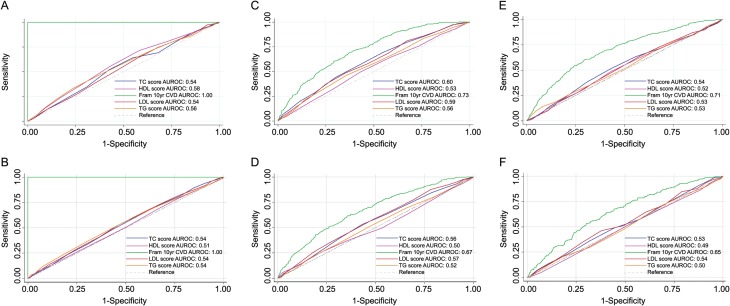
Methods and results: Analysis was performed in two prospective cohorts: Whitehall II (WHII; N = 5059) and the British Women's Heart and Health Study (BWHHS; N = 3414). For each participant, scores were calculated based on the cumulative effect of multiple genetic variants influencing total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglycerides (TG). Compared with the bottom quintile, individuals in the top quintile of the LDL-C genetic score distribution had higher LDL-C {mean difference of 0.85 [95% confidence interval, (CI) = 0.76-0.94] and 0.63 [95% CI = 0.50-0.76] mmol/l in WHII and BWHHS, respectively}. They also tended to have greater odds of having 'high-risk' status (Framingham 10-year cardiovascular disease risk >20%) [WHII: odds ratio (OR) = 1.36 (0.93-1.98), BWHHS: OR = 1.49 (1.14-1.94)]; receiving lipid-lowering treatment [WHII: OR = 2.38 (1.57-3.59), BWHHS: OR = 2.24 (1.52-3.29)]; and CHD events [WHII: OR = 1.43 (1.02-2.00), BWHHS: OR = 1.31 (0.99-1.72)]. Similar associations were observed for the TC score in both studies. The TG score was associated with high-risk status and medication use in both studies. Neither HDL nor TG scores were associated with the risk of coronary events. The genetic scores did not improve discrimination over the Framingham risk score.
Conclusion: At the population level, common SNPs associated with LDL-C and TC contribute to blood lipid variation, cardiovascular risk, use of lipid-lowering medications and coronary events. However, their effects are too small to discriminate future lipid-lowering medication requirements or coronary events.
Figures
Comment in
-
Genes and cardiovascular risk.Eur Heart J. 2013 Apr;34(13):949-50. doi: 10.1093/eurheartj/ehs439. Epub 2012 Dec 19. Eur Heart J. 2013. PMID: 23257949 No abstract available.
Similar articles
-
Genetic Association of Lipids and Lipid Drug Targets With Abdominal Aortic Aneurysm: A Meta-analysis.JAMA Cardiol. 2018 Jan 1;3(1):26-33. doi: 10.1001/jamacardio.2017.4293. JAMA Cardiol. 2018. PMID: 29188294 Free PMC article. Review.
-
Evaluating the relationship between circulating lipoprotein lipids and apolipoproteins with risk of coronary heart disease: A multivariable Mendelian randomisation analysis.PLoS Med. 2020 Mar 23;17(3):e1003062. doi: 10.1371/journal.pmed.1003062. eCollection 2020 Mar. PLoS Med. 2020. PMID: 32203549 Free PMC article.
-
Polymorphisms associated with cholesterol and risk of cardiovascular events.N Engl J Med. 2008 Mar 20;358(12):1240-9. doi: 10.1056/NEJMoa0706728. N Engl J Med. 2008. PMID: 18354102
-
Mendelian randomization of blood lipids for coronary heart disease.Eur Heart J. 2015 Mar 1;36(9):539-50. doi: 10.1093/eurheartj/eht571. Epub 2014 Jan 27. Eur Heart J. 2015. PMID: 24474739 Free PMC article.
-
Identifying patients at risk for coronary heart disease: implications from trials of lipid-lowering drug therapy.QJM. 2000 Sep;93(9):567-74. doi: 10.1093/qjmed/93.9.567. QJM. 2000. PMID: 10984551 Review.
Cited by
-
Risk prediction by genetic risk scores for coronary heart disease is independent of self-reported family history.Eur Heart J. 2016 Feb 7;37(6):561-7. doi: 10.1093/eurheartj/ehv462. Epub 2015 Sep 20. Eur Heart J. 2016. PMID: 26392438 Free PMC article.
-
Excessive fuel availability amplifies the FTO-mediated obesity risk: results from the TUEF and Whitehall II studies.Sci Rep. 2017 Nov 14;7(1):15486. doi: 10.1038/s41598-017-15744-4. Sci Rep. 2017. PMID: 29138452 Free PMC article.
-
Novel genetic loci associated with long-term deterioration in blood lipid concentrations and coronary artery disease in European adults.Int J Epidemiol. 2017 Aug 1;46(4):1211-1222. doi: 10.1093/ije/dyw245. Int J Epidemiol. 2017. PMID: 27864399 Free PMC article.
-
Associations of genetic variants for adult lipid levels with lipid levels in children. The Generation R Study.J Lipid Res. 2016 Dec;57(12):2185-2192. doi: 10.1194/jlr.P066902. Epub 2016 Oct 24. J Lipid Res. 2016. PMID: 27777320 Free PMC article.
-
Impact of HDL genetic risk scores on coronary artery calcified plaque and mortality in individuals with type 2 diabetes from the Diabetes Heart Study.Cardiovasc Diabetol. 2013 Jun 25;12:95. doi: 10.1186/1475-2840-12-95. Cardiovasc Diabetol. 2013. PMID: 23799899 Free PMC article.
References
-
- Baigent C, Blackwell L, Emberson J, Holland L, Reith C, Bhala N, Peto R, Barnes EH, Keech A, Simes J, Collins R. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170 000 participants in 26 randomised trials. Lancet. 2010;376:1670–1681. doi:10.1016/S0140-6736(10)61350-5. - DOI - PMC - PubMed
-
- Emberson JR, Whincup PH, Morris RW, Walker M. Re-assessing the contribution of serum total cholesterol, blood pressure and cigarette smoking to the aetiology of coronary heart disease: impact of regression dilution bias. Eur Heart J. 2003;24:1719–1726. doi:10.1016/S0195-668X(03)00471-8. - DOI - PubMed
-
- Law MR, Wald NJ. Risk factor thresholds: their existence under scrutiny. BMJ. 2002;324:1570–1576. doi:10.1136/bmj.324.7353.1570. - DOI - PMC - PubMed
-
- Di Angelantonio E, Sarwar N, Perry P, Kaptoge S, Ray KK, Thompson A, Wood AM, Lewington S, Sattar N, Packard CJ, Collins R, Thompson SG, Danesh J. Major lipids, apolipoproteins, and risk of vascular disease. JAMA. 2009;302:1993–2000. doi:10.1001/jama.2009.1619. - DOI - PMC - PubMed
-
- Anderson KM, Odell PM, Wilson PW, Kannel WB. Cardiovascular disease risk profiles. Am Heart J. 1991;121:293–298. doi:10.1016/0002-8703(91)90861-B. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
