

Comparison between different thickness umbrella-shaped expandable radiofrequency electrodes (SuperSlim and CoAccess): Experimental and clinical study
- PMID: 22977647
- PMCID: PMC3440824
- DOI: 10.3892/etm.2011.347
Comparison between different thickness umbrella-shaped expandable radiofrequency electrodes (SuperSlim and CoAccess): Experimental and clinical study
Abstract
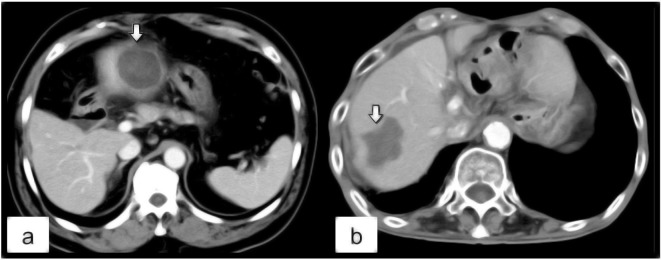
The purpose of the present study was to compare the size and configuration of the ablation zones created by SuperSlim and CoAccess electrodes, using various ablation algorithms in ex vivo bovine liver and in clinical cases. In the experimental study, we ablated explanted bovine liver using 2 types of electrodes and 4 ablation algorithms (combinations of incremental power supply, stepwise expansion and additional low-power ablation) and evaluated the ablation area and time. In the clinical study, we compared the ablation volume and the shape of the ablation zone between both electrodes in 23 hepatocellular carcinoma (HCC) cases with the best algorithm (incremental power supply, stepwise expansion and additional low-power ablation) as derived from the experimental study. In the experimental study, the ablation area and time by the CoAccess electrode were significantly greater compared to those by the SuperSlim electrode for the single-step (algorithm 1, p=0.0209 and 0.0325, respectively) and stepwise expansion algorithms (algorithm 2, p=0.0002 and <0.0001, respectively; algorithm 3, p= 0.006 and 0.0407, respectively). However, differences were not significant for the additional low-power ablation algorithm. In the clinical study, the ablation volume and time in the CoAccess group were significantly larger and longer, respectively, compared to those in the SuperSlim group (p=0.0242 and 0.009, respectively). Round ablation zones were acquired in 91.7% of the CoAccess group, while irregular ablation zones were obtained in 45.5% of the SuperSlim group (p=0.0428). In conclusion, the CoAccess electrode achieves larger and more uniform ablation zones compared with the SuperSlim electrode, though it requires longer ablation times in experimental and clinical studies.
Figures


References
-
- Gervais DA, Goldberg SN, Brown DB, Soulen MC, Millward SF, Rajan DK. Society of interventional radiology position statement on percutaneous radiofrequency ablation for the treatment of liver tumors. J Vasc Interv Radiol. 2000;20:3–8. - PubMed
-
- Livraghi T, Meloni F, Di Stasi M, et al. Sustained complete response and complications rates after radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: is resection still the treatment of choice? Hepatology. 2008;47:82–89. - PubMed
-
- Bhardwaj N, Strickland AD, Ahmad F, Dennison AR, Lloyd DM. Liver ablation techniques: a review. Surg Endosc. 2010;24:254–265. - PubMed
LinkOut - more resources
Full Text Sources