

Indications, Knives, and Electric Current: What's the Best?
- PMID: 22977819
- PMCID: PMC3429753
- DOI: 10.5946/ce.2012.45.3.285
Indications, Knives, and Electric Current: What's the Best?
Abstract
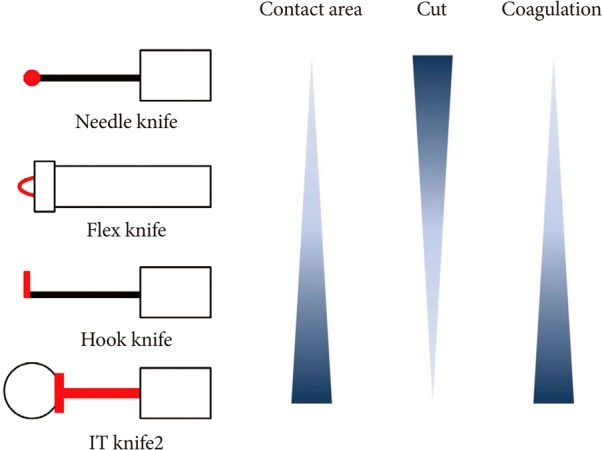
Endoscopic submucosal dissection (ESD) was developed to overcome the limitations of conventional endoscopic mucosal resection (EMR), and ESD has been also applied for large colorectal neoplasms. Since colorectal ESD is still associated with higher perforation rate, a longer procedure time, and increased technical difficulty, the indications should be strictly considered. Generally, colorectal tumors without deep submucosal invasion or minimal possibility of lymph node metastasis, for which en bloc resection using conventional EMR is difficult, are good candidates for colorectal ESD. The ideal knife for colorectal ESD should avoid making perforations but can make a clean cut of optimal depth at one time. The ideal current for ESD differs depending on the procedure used, the surgical devices used, the tissue to be dissected, and the operator's preference. Application of the optimal indications and improvements in the technical skill and surgical devices are required for easier and safer colorectal ESD.
Keywords: Colonoscopy; Colorectal neoplasms; Endoscopic submucosal dissection.
Conflict of interest statement
The author has no financial conflicts of interest.
Figures
Similar articles
-
Endoscopic treatment for early stage colorectal tumors: the comparison between EMR with small incision, simplified ESD, and ESD using the standard flush knife and the ball tipped flush knife.Acta Chir Iugosl. 2010;57(3):41-6. doi: 10.2298/aci1003041t. Acta Chir Iugosl. 2010. PMID: 21066982
-
Colorectal endoscopic submucosal dissection: Technical advantages compared to endoscopic mucosal resection and minimally invasive surgery.Dig Endosc. 2014 Jan;26 Suppl 1:52-61. doi: 10.1111/den.12196. Epub 2013 Nov 5. Dig Endosc. 2014. PMID: 24191896 Review.
-
AGA Institute Clinical Practice Update: Endoscopic Submucosal Dissection in the United States.Clin Gastroenterol Hepatol. 2019 Jan;17(1):16-25.e1. doi: 10.1016/j.cgh.2018.07.041. Epub 2018 Aug 2. Clin Gastroenterol Hepatol. 2019. PMID: 30077787 Review.
-
Efficacy of hybrid endoscopic submucosal dissection (ESD) as a rescue treatment in difficult colorectal ESD cases.Dig Endosc. 2017 Apr;29 Suppl 2:45-52. doi: 10.1111/den.12863. Dig Endosc. 2017. PMID: 28425649
-
Clinical outcome of endoscopic submucosal dissection versus endoscopic mucosal resection of large colorectal tumors as determined by curative resection.Surg Endosc. 2010 Feb;24(2):343-52. doi: 10.1007/s00464-009-0562-8. Epub 2009 Jun 11. Surg Endosc. 2010. PMID: 19517168
Cited by
-
International digestive endoscopy network to strengthen network for lower gastrointestinal diseases including inflammatory bowel disease and colorectal cancer.Clin Endosc. 2012 Sep;45(3):251-3. doi: 10.5946/ce.2012.45.3.251. Epub 2012 Aug 22. Clin Endosc. 2012. PMID: 22977812 Free PMC article.
-
Colorectal Endoscopic Submucosal Dissection: Past, Present, and Factors Impacting Future Dissemination.Clin Colon Rectal Surg. 2015 Sep;28(3):146-51. doi: 10.1055/s-0035-1555006. Clin Colon Rectal Surg. 2015. PMID: 26491406 Free PMC article. Review.
References
-
- Saito Y, Uraoka T, Matsuda T, et al. Endoscopic treatment of large superficial colorectal tumors: a case series of 200 endoscopic submucosal dissections (with video) Gastrointest Endosc. 2007;66:966–973. - PubMed
-
- Fujishiro M, Yahagi N, Kakushima N, et al. Outcomes of endoscopic submucosal dissection for colorectal epithelial neoplasms in 200 consecutive cases. Clin Gastroenterol Hepatol. 2007;5:678–683. - PubMed
-
- Toyonaga T, Man-i M, Fujita T, et al. Retrospective study of technical aspects and complications of endoscopic submucosal dissection for laterally spreading tumors of the colorectum. Endoscopy. 2010;42:714–722. - PubMed
-
- Kitajima K, Fujimori T, Fujii S, et al. Correlations between lymph node metastasis and depth of submucosal invasion in submucosal invasive colorectal carcinoma: a Japanese collaborative study. J Gastroenterol. 2004;39:534–543. - PubMed
-
- Ueno H, Mochizuki H, Hashiguchi Y, et al. Risk factors for an adverse outcome in early invasive colorectal carcinoma. Gastroenterology. 2004;127:385–394. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
