

Family history of alcohol dependence and antidepressant response to an N-methyl-D-aspartate antagonist in bipolar depression
- PMID: 22978511
- PMCID: PMC3504126
- DOI: 10.1111/bdi.12003
Family history of alcohol dependence and antidepressant response to an N-methyl-D-aspartate antagonist in bipolar depression
Abstract
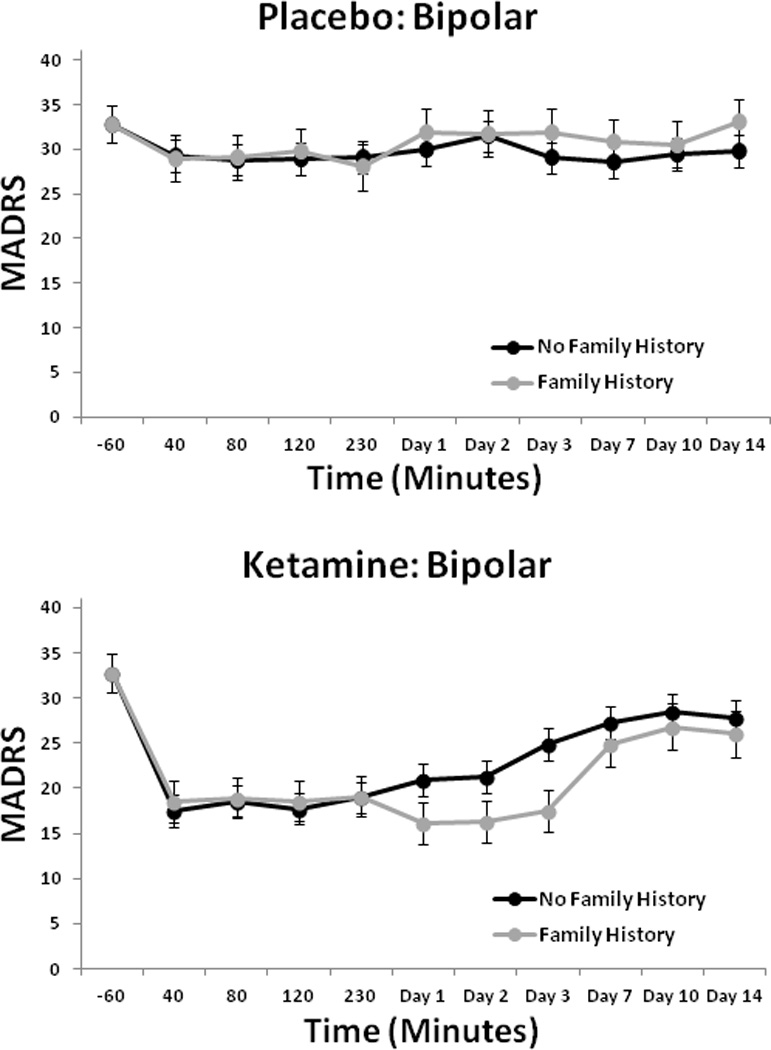
Objectives: Both ketamine and ethanol are N-methyl-d-aspartate (NMDA) receptor antagonists. Ketamine has rapid antidepressant properties in major depressive disorder (MDD) as well as bipolar depression. In individuals with MDD, a positive family history of alcohol dependence (FHP) was associated with greater improvement in depressive symptoms after ketamine administration compared to individuals whose family history of alcohol dependence was negative (FHN). This study investigated whether FHP influences ketamine's antidepressant and perceptual effects in individuals with bipolar depression.
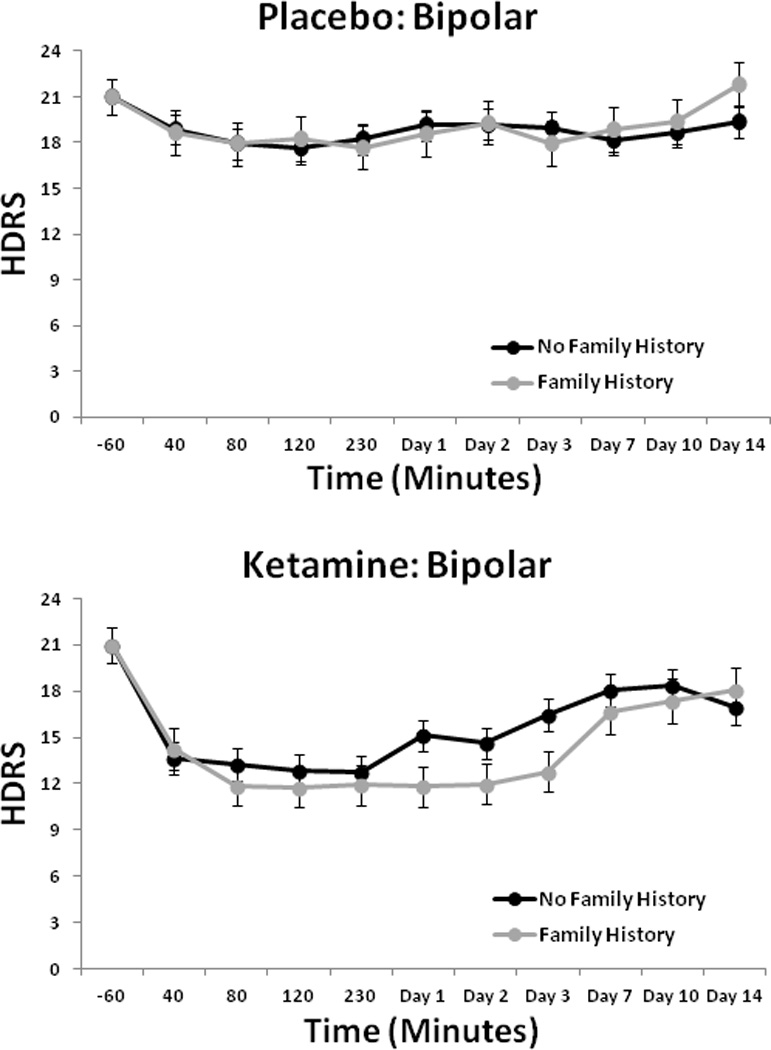
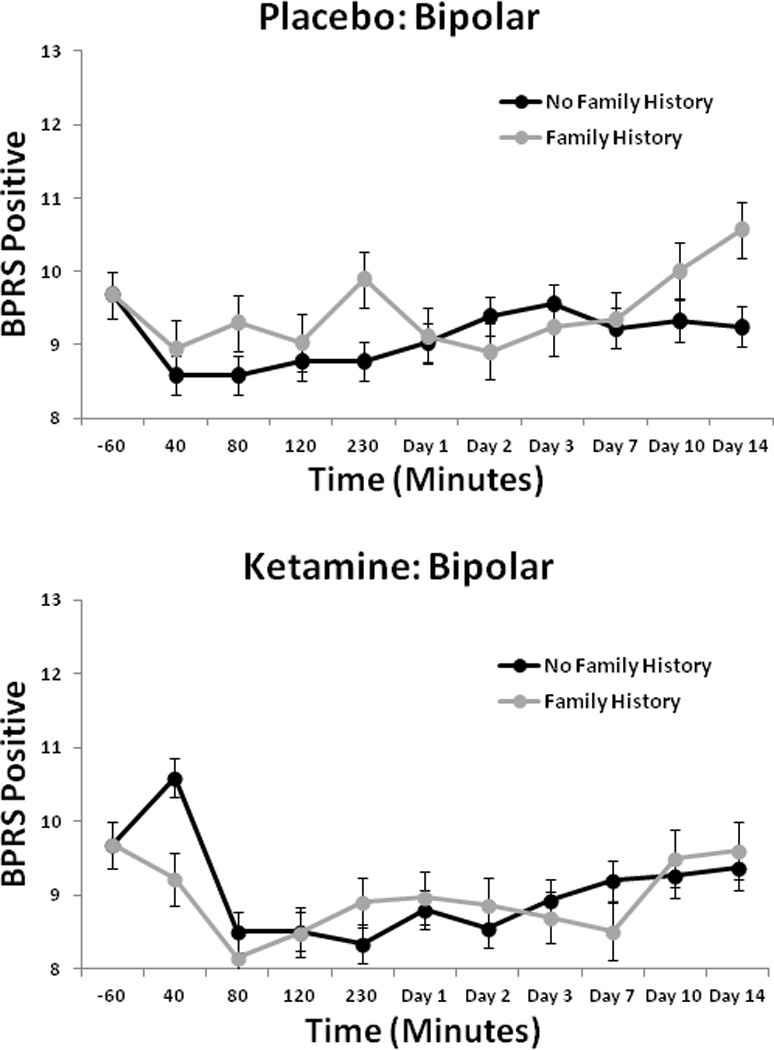
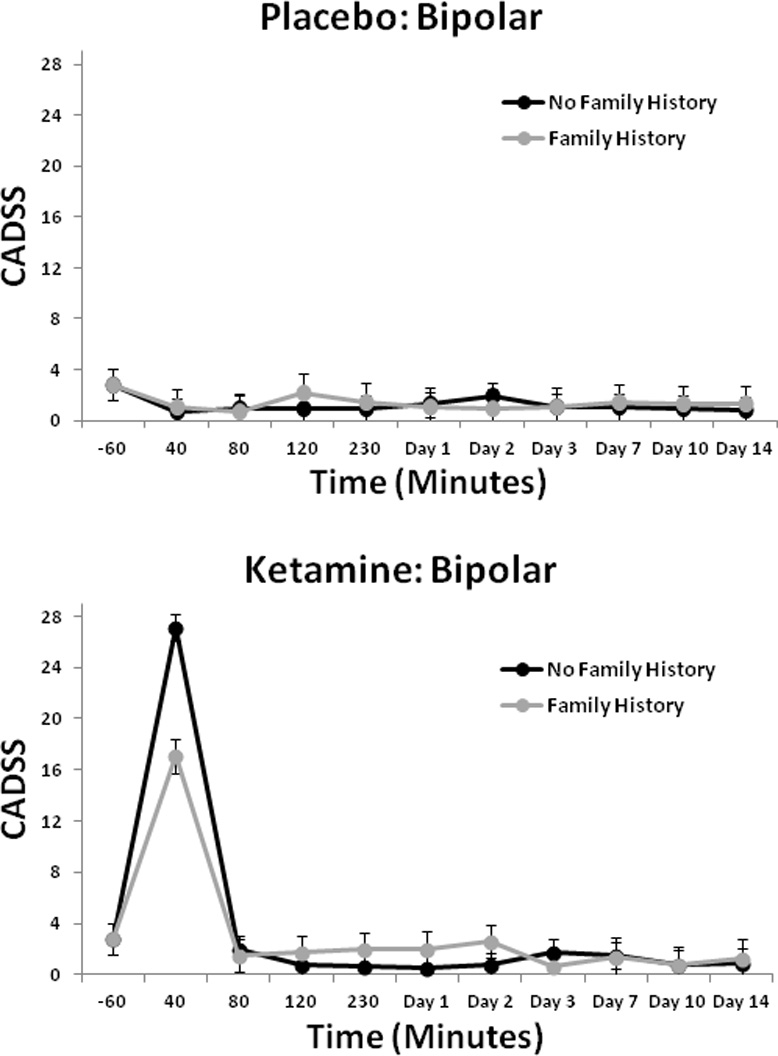
Methods: A post hoc analysis was conducted on 33 subjects with DSM-IV bipolar disorder (BD) type I or II depression pooled from two previously published studies. All subjects had undergone a double-blind, randomized, crossover trial of a single intravenous infusion of ketamine (0.5 mg/kg) combined with lithium or valproate therapy. Subjects were rated at baseline; at 40, 80, 120, and 230 min; and at days 1, 2, 3, 7, 10, and 14 post-infusion. The primary outcome measure was Montgomery-Åsberg Depression Rating Scale (MADRS) scores. Patients were categorized as FHP when they reported at least one first-degree relative with alcohol dependence. Measures of psychosis, dissociation, and dysphoria were also collected.
Results: After ketamine infusion, subjects with FHP showed significantly greater improvement on MADRS scores than FHN subjects. In addition, patients with FHP had attenuated psychotomimetic and dissociative scores compared to FHN patients.
Conclusions: FHP appears to predict a more sustained antidepressant response to ketamine in individuals with BD. Family history of alcoholism may be an important consideration in the development of glutamatergic-based therapies for depression.
Published 2012. This article is a U.S. Government work and is in the public domain in the USA.
Conflict of interest statement
A patent application for the use of ketamine in depression has been submitted listing CAZ among the inventors; he has assigned his rights on the patent to the U.S. Government but will share a percentage of any royalties that may be received by the government. DAL, LI, NB, JF-C, DM, CAM, and CC have no conflicts of interest to disclose, financial or otherwise.
Figures
Similar articles
-
Ketamine's antidepressant efficacy is extended for at least four weeks in subjects with a family history of an alcohol use disorder.Int J Neuropsychopharmacol. 2014 Oct 31;18(1):pyu039. doi: 10.1093/ijnp/pyu039. Int J Neuropsychopharmacol. 2014. PMID: 25539512 Free PMC article. Clinical Trial.
-
Symptomatology and predictors of antidepressant efficacy in extended responders to a single ketamine infusion.J Affect Disord. 2017 Jan 15;208:560-566. doi: 10.1016/j.jad.2016.10.026. Epub 2016 Oct 26. J Affect Disord. 2017. PMID: 27839782 Free PMC article. Review.
-
Family history of alcohol dependence and initial antidepressant response to an N-methyl-D-aspartate antagonist.Biol Psychiatry. 2009 Jan 15;65(2):181-4. doi: 10.1016/j.biopsych.2008.09.029. Epub 2008 Nov 8. Biol Psychiatry. 2009. PMID: 18996507 Free PMC article. Clinical Trial.
-
A randomized add-on trial of an N-methyl-D-aspartate antagonist in treatment-resistant bipolar depression.Arch Gen Psychiatry. 2010 Aug;67(8):793-802. doi: 10.1001/archgenpsychiatry.2010.90. Arch Gen Psychiatry. 2010. PMID: 20679587 Free PMC article. Clinical Trial.
-
[Ketamine for treatment of acute depression].Ugeskr Laeger. 2013 Sep 9;175(37):2090-3. Ugeskr Laeger. 2013. PMID: 24011203 Review. Danish.
Cited by
-
Anti-anhedonic effect of ketamine and its neural correlates in treatment-resistant bipolar depression.Transl Psychiatry. 2014 Oct 14;4(10):e469. doi: 10.1038/tp.2014.105. Transl Psychiatry. 2014. PMID: 25313512 Free PMC article. Clinical Trial.
-
Clinical predictors of ketamine response in treatment-resistant major depression.J Clin Psychiatry. 2014 May;75(5):e417-23. doi: 10.4088/JCP.13m08698. J Clin Psychiatry. 2014. PMID: 24922494 Free PMC article. Clinical Trial.
-
Efficacy of ketamine for major depressive episodes at 2, 4, and 6-weeks post-treatment: A meta-analysis.Psychopharmacology (Berl). 2021 Jul;238(7):1737-1752. doi: 10.1007/s00213-021-05825-8. Epub 2021 Mar 31. Psychopharmacology (Berl). 2021. PMID: 33787963 Review.
-
Neural correlates of change in major depressive disorder anhedonia following open-label ketamine.J Psychopharmacol. 2015 May;29(5):596-607. doi: 10.1177/0269881114568041. Epub 2015 Feb 17. J Psychopharmacol. 2015. PMID: 25691504 Free PMC article. Clinical Trial.
-
Predictors of Response to Ketamine in Treatment Resistant Major Depressive Disorder and Bipolar Disorder.Int J Environ Res Public Health. 2018 Apr 17;15(4):771. doi: 10.3390/ijerph15040771. Int J Environ Res Public Health. 2018. PMID: 29673146 Free PMC article. Review.
References
-
- Salloum IM, Thase ME. Impact of substance abuse on the course and treatment of bipolar disorder. Bipolar Disord. 2000;2:269–280. - PubMed
-
- Black DW, Winokur G, Nasrallah A. Mortality in patients with primary unipolar depression, secondary unipolar depression, and bipolar affective disorder: a comparison with general population mortality. Int J Psychiatry Med. 1987;17:351–360. - PubMed
-
- Brady KT, Lydiard RB. Bipolar affective disorder and substance abuse. J Clin Psychopharmacol. 1992;12:17S–22S. - PubMed
