

Adipose tissue invariant NKT cells protect against diet-induced obesity and metabolic disorder through regulatory cytokine production
- PMID: 22981538
- PMCID: PMC4991771
- DOI: 10.1016/j.immuni.2012.06.016
Adipose tissue invariant NKT cells protect against diet-induced obesity and metabolic disorder through regulatory cytokine production
Abstract
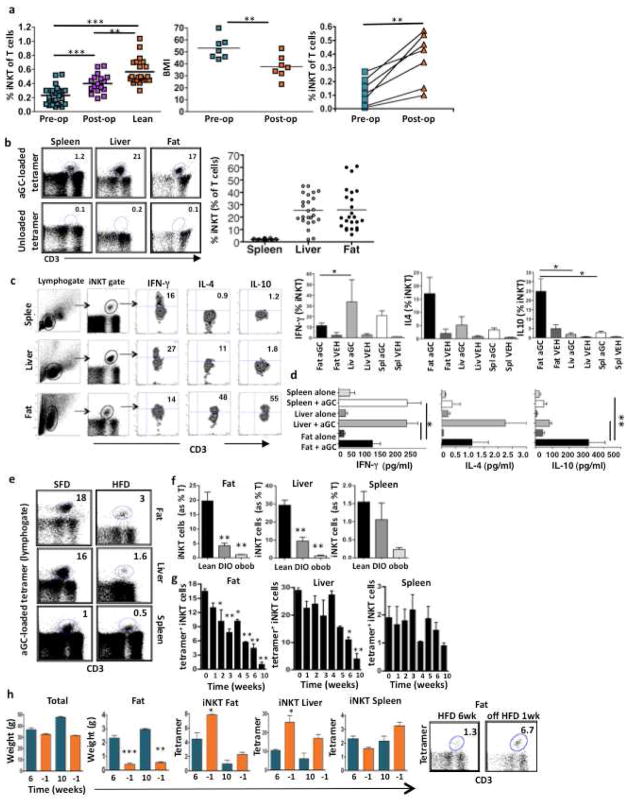
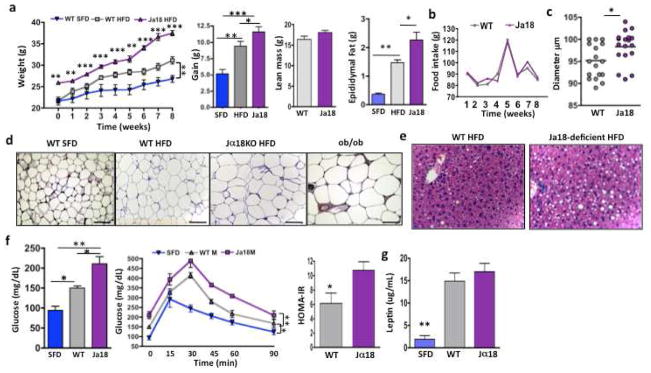
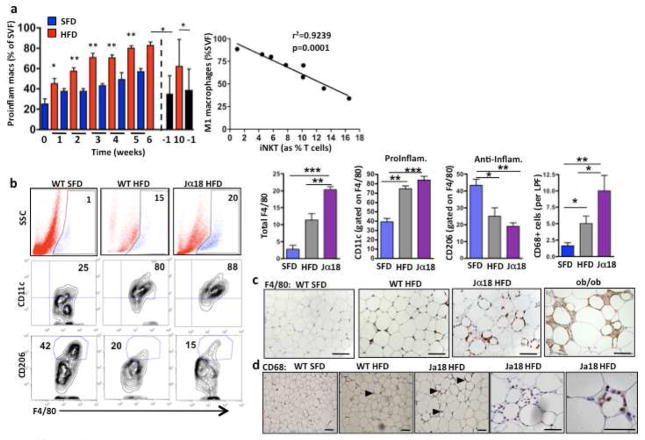
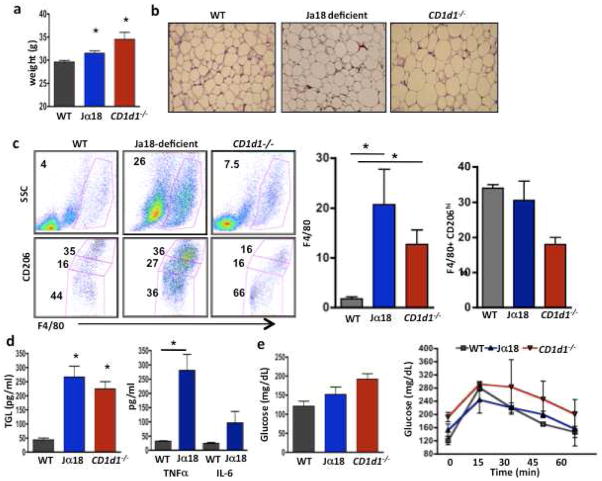
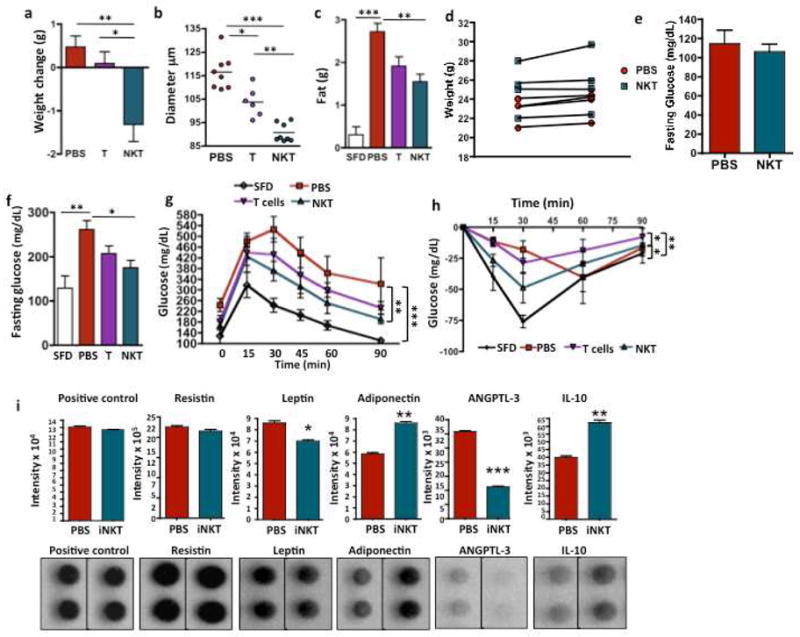
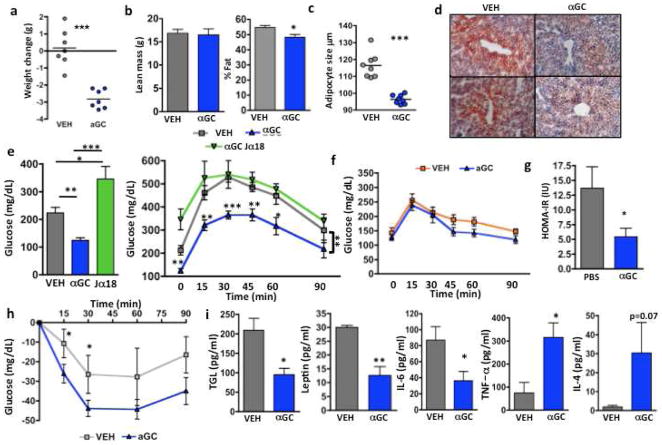
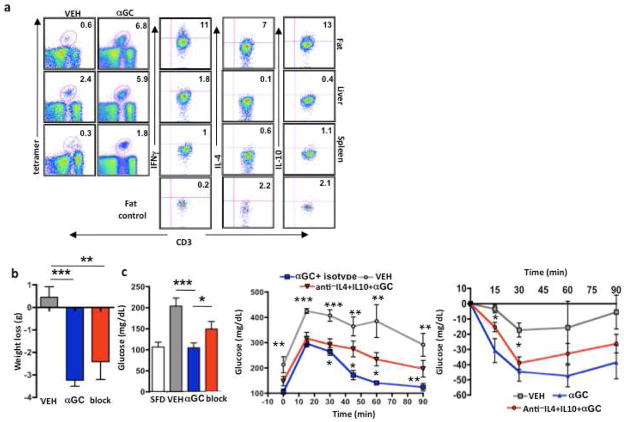
Invariant natural killer T (iNKT) cells are evolutionarily conserved innate T cells that influence inflammatory responses. We have shown that iNKT cells, previously thought to be rare in humans, were highly enriched in human and murine adipose tissue, and that as adipose tissue expanded in obesity, iNKT cells were depleted, correlating with proinflammatory macrophage infiltration. iNKT cell numbers were restored in mice and humans after weight loss. Mice lacking iNKT cells had enhanced weight gain, larger adipocytes, fatty livers, and insulin resistance on a high-fat diet. Adoptive transfer of iNKT cells into obese mice or in vivo activation of iNKT cells via their lipid ligand, alpha-galactocylceramide, decreased body fat, triglyceride levels, leptin, and fatty liver and improved insulin sensitivity through anti-inflammatory cytokine production by adipose-derived iNKT cells. This finding highlights the potential of iNKT cell-targeted therapies, previously proven to be safe in humans, in the management of obesity and its consequences.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
The other authors have no conflicting financial interests.
Figures
Comment in
-
Fat chance: not much against NKT cells.Immunity. 2012 Sep 21;37(3):447-9. doi: 10.1016/j.immuni.2012.09.006. Immunity. 2012. PMID: 22999952
References
-
- Bendelac A, Savage PB, Teyton L. The biology of NKT cells. Annu Rev Immunol. 2007;25:297–336. - PubMed
-
- Berzins SP, Smyth MJ, Baxter AG. Presumed guilty: natural killer T cell defects and human disease. Nat Rev Immunol. 11:131–142. - PubMed
-
- Brigl M, Brenner MB. CD1: antigen presentation and T cell function. Annu Rev Immunol. 2004;22:817–890. - PubMed
-
- Cerundolo V, Silk JD, Masri SH, Salio M. Harnessing invariant NKT cells in vaccination strategies. Nat Rev Immunol. 2009;9:28–38. - PubMed
-
- Dalmas E, Clement K, Guerre-Millo M. Defining macrophage phenotype and function in adipose tissue. Trends Immunol 2011 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
