

Massive neonatal adrenal enlargement due to cytomegaly, persistence of the transient cortex, and hyperplasia of the permanent cortex: findings in Cushing syndrome associated with hemihypertrophy
- PMID: 22982888
- PMCID: PMC3444746
- DOI: 10.1097/PAS.0b013e31825d538b
Massive neonatal adrenal enlargement due to cytomegaly, persistence of the transient cortex, and hyperplasia of the permanent cortex: findings in Cushing syndrome associated with hemihypertrophy
Abstract
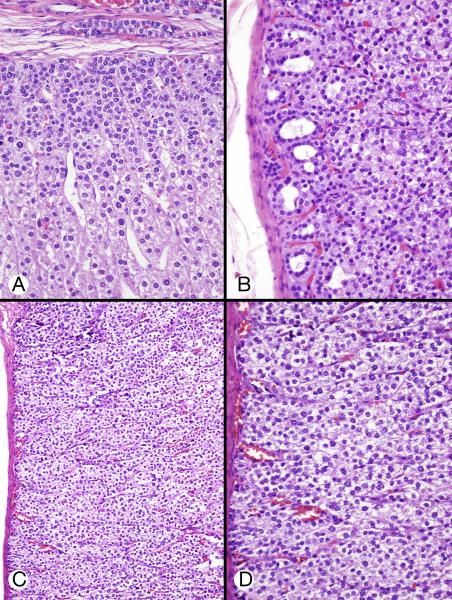
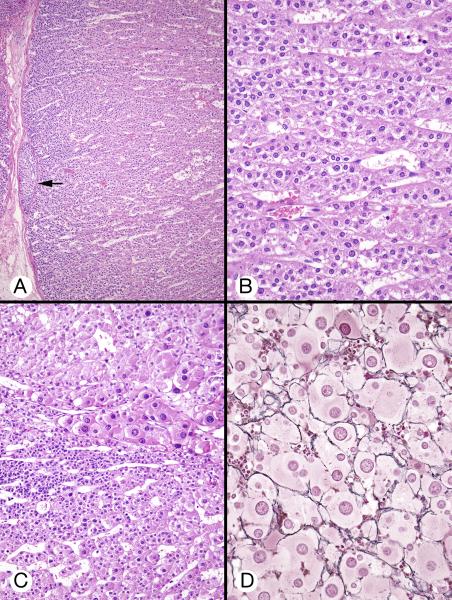
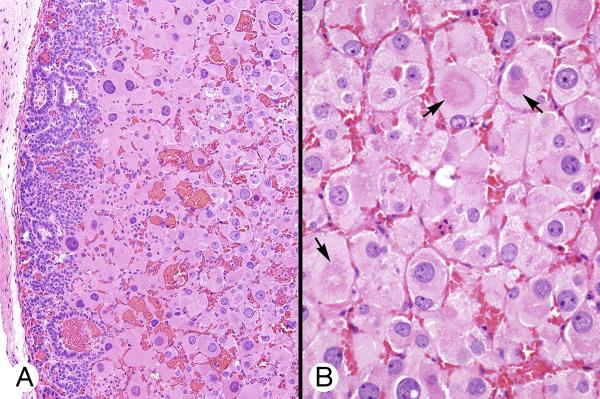
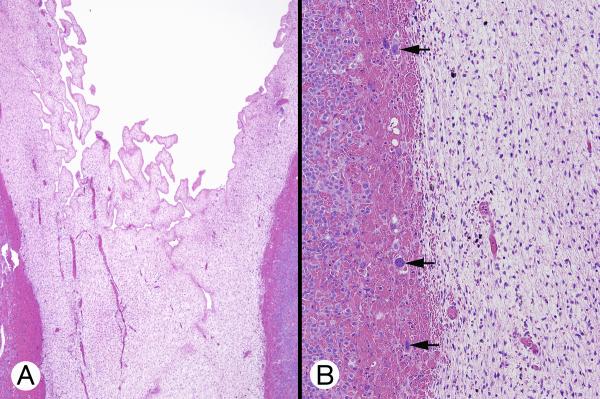
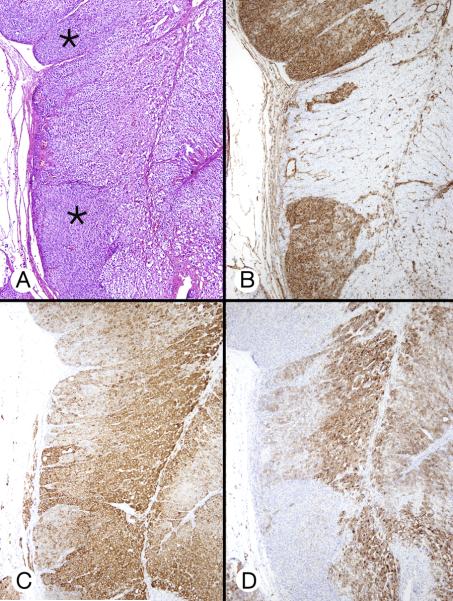
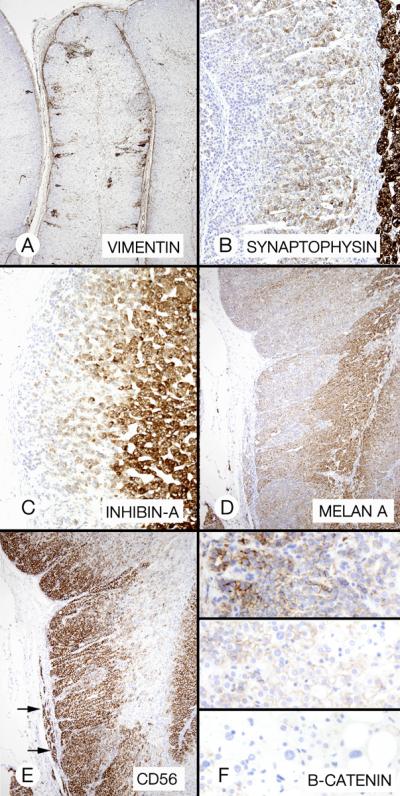
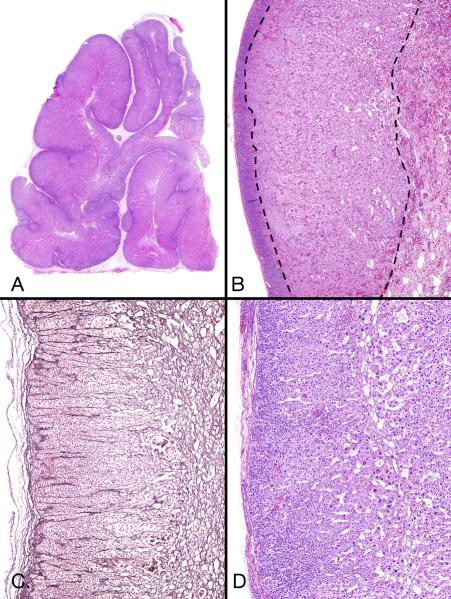
Described in this article is the massive enlargement of both adrenal glands in 3 newborns-2 girls and 1 boy. Two had hemihypertrophy and other congenital abnormalities but no identified genetic mutation; the third had genetically proven Beckwith-Wiedemann syndrome. Two had severe Cushing syndrome, the third had hypercortisolemia but no clinical Cushing syndrome. Bilateral adrenalectomy cured Cushing syndrome in the 2 with severe symptoms; total adrenal weight in these patients was 44 and 53 g, respectively. Unilateral adrenalectomy was performed in the third patient: the gland weighed 52 g; postoperatively, the patient's hypercortisolemia normalized, and, concomitantly, the enlarged contralateral adrenal gland had a 5-fold decrease in size with slight enlargement 6 years postoperatively. Microscopically, the 3 patients had similar pathology: massive adrenal enlargement due to a combination of cytomegaly, persistence of the transient cortex, and hyperplasia of the permanent cortex. The pathologic findings were most likely the result of the genetic mutation identified in 1 patient and of an unknown mutation in the remaining 2 patients.
Figures

References
-
- Aterman K, Kerenyi N, Lee M. Adrenal cytomegaly. Virchows Arch Abt A Path Anat. 1972;355:105–122. - PubMed
-
- Beckwith JB. Macroglossia, omphalocele, adrenal cytomegaly, gigantism, and hyperplastic visceromegaly. Birth Defects. 1969;5:188–196.
-
- Borit A, Kosek J. Cytomegaly of the adrenal cortex: Electron microscopy in Beckwith's syndrome. Arch Pathol Lab Med. 1969;88:58–64. - PubMed
-
- Carney JA. Adrenal Gland. In: Mills SE, editor. Histology for Pathologists. 4th edition. Lippincott, Williams and Wilkins; Philadelphia, PA: 2012. in press.
