

Lumbar spine MRI in upright position for diagnosing acute and chronic low back pain: statistical analysis of morphological changes
- PMID: 22983676
- PMCID: PMC3585839
- DOI: 10.1007/s10195-012-0213-z
Lumbar spine MRI in upright position for diagnosing acute and chronic low back pain: statistical analysis of morphological changes
Abstract
Background: Patients with low back pain frequently demonstrate recumbent magnetic resonance imaging (MRI) alterations not always related to homogeneous clinical symptoms. The purpose of this study was to evaluate and quantify the statistical significance of variations of some anatomical parameters of the lumbosacral spine and reveal occult disc pathologies from recumbent to upright position in patients with acute and chronic low back pain.
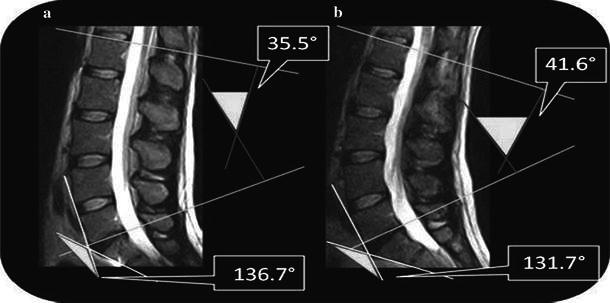
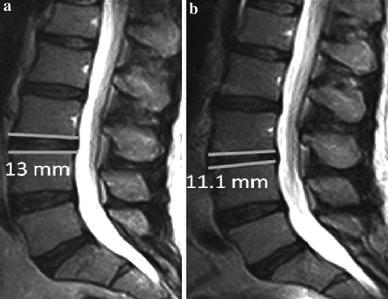
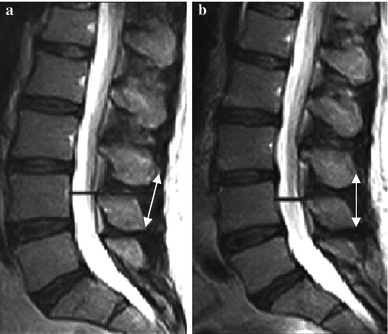
Materials and methods: Fifty-seven patients complaining of low back pain (27 women, 30 men) underwent dynamic lumbosacral MRI with a 0.25-T tilting system (G-scan Esaote). We settled five parameters for which variations have been evaluated: lumbosacral angle, lordosis angle, L3-L4 intersomatic disc height, L3-L4 interspinous processes distance, and widest anteroposterior dural sac diameter. Images were obtained in both recumbent and upright positions.
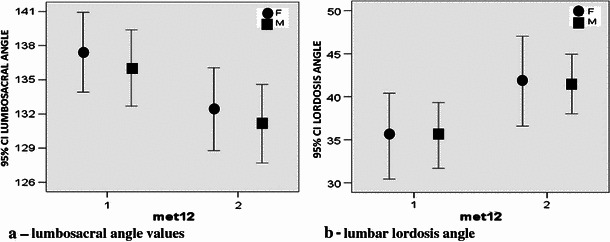
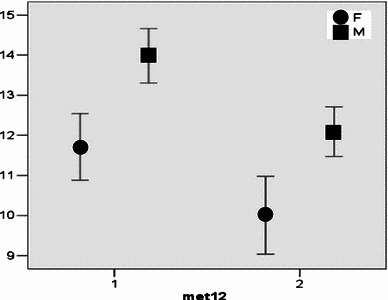
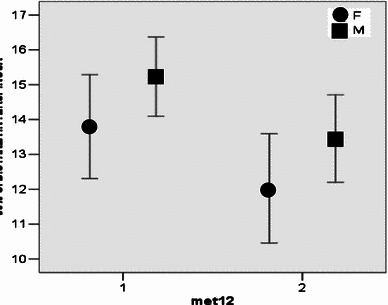
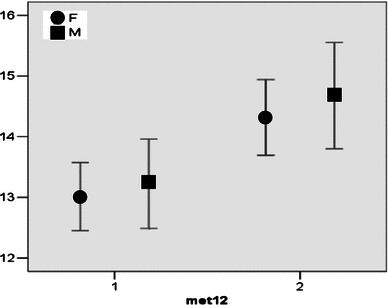
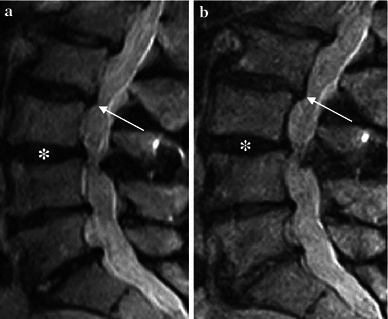
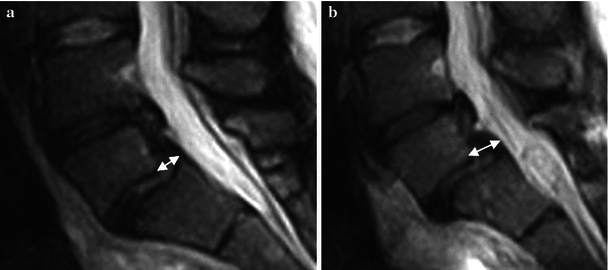
Results: Statistically significant differences [one-way analysis of variance (ANOVA), p = 0.0043] were found between each pair of values of parameters sampled in recumbent and upright positions. In 70 % of patients, on visual qualitative analysis only, an increment of disc protrusions and/or spondylolisthesis was found in the upright position; in three cases, in the upright position only, an interarticular pseudocyst was found.
Conclusions: Dynamic MRI with an open-configuration, low-field tilting MRI system is a feasible and promising tool to study degenerative pathology of the spine. Moreover, in cases of low back pain with negative MRI in the recumbent position or in patients with pain in the upright position only, tilting MRI permits visualization of occult spine and disc pathologies in patients with acute or chronic low back pain.
Figures

References
-
- Splendiani A, Di Fabio MV, Barile A, Masciocchi C. Tecnica di studio RM del rachide lombare sotto carico. In: Leone A, Martino F, editors. Imaging del rachide. Il vecchio e il nuovo. Italy: Springer; 2008. pp. 123–134.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
