

PET/MR for therapy response evaluation in malignant lymphoma: initial experience
- PMID: 22983794
- PMCID: PMC3572376
- DOI: 10.1007/s10334-012-0342-7
PET/MR for therapy response evaluation in malignant lymphoma: initial experience
Abstract
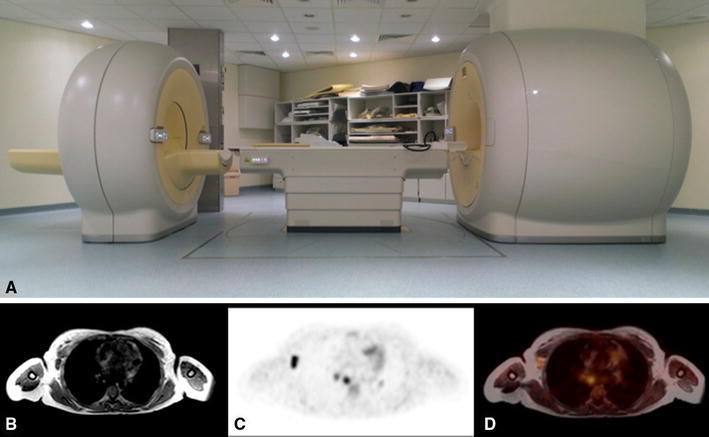
Object: To evaluate the feasibility of positron emission tomography/magnetic resonance imaging (PET/MR) with (18)fluoro-2-deoxyglucose (FDG) for therapy response evaluation of malignant lymphoma.
Materials and methods: Nine patients with malignant lymphoma who underwent FDG-PET/MR before and after chemotherapy were included in this retrospective study. Average time between the two scans was 70 days. The scans were evaluated independently by two nuclear medicine physicians. The Ann Arbor classification was used to describe lymphoma stage. Furthermore, the readers also rated PET image quality using a five point scale. Weighted kappa (κ) was used to calculate interrater agreement.
Results: The initial scan showed foci of increased FDG uptake in all patients, with Ann Arbor stage varying between I and IV. In the follow-up examination, all but one patient showed complete response to chemotherapy. PET image quality was rated as very good or excellent for all scans. Interrater agreement was excellent regarding Ann Arbor stage (κ = 0.97) and good regarding image quality (κ = 0.41).
Conclusion: PET/MR shows promising initial results for therapy response evaluation in lymphoma patients.
Figures



References
-
- Swerdlow SH, International Agency for Research on Cancer, World Health Organization (2008) WHO classification of tumours of haematopoietic and lymphoid tissues. World Health Organization classification of tumours, 4th edn. International Agency for Research on Cancer, Lyon, France
-
- Juweid ME, Stroobants S, Hoekstra OS, Mottaghy FM, Dietlein M, Guermazi A, Wiseman GA, Kostakoglu L, Scheidhauer K, Buck A, Naumann R, Spaepen K, Hicks RJ, Weber WA, Reske SN, Schwaiger M, Schwartz LH, Zijlstra JM, Siegel BA, Cheson BD. Use of positron emission tomography for response assessment of lymphoma: consensus of the Imaging Subcommittee of International Harmonization Project in Lymphoma. J Clin Oncol. 2007;25(5):571–578. doi: 10.1200/JCO.2006.08.2305. - DOI - PubMed
-
- Czernin J, Allen-Auerbach M, Schelbert HR. Improvements in cancer staging with PET/CT: literature-based evidence as of September 2006. J Nucl Med. 2007;48(Suppl 1):78S–88S. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
