

Biological determinants linking infant weight gain and child obesity: current knowledge and future directions
- PMID: 22983846
- PMCID: PMC3648749
- DOI: 10.3945/an.112.002238
Biological determinants linking infant weight gain and child obesity: current knowledge and future directions
Abstract
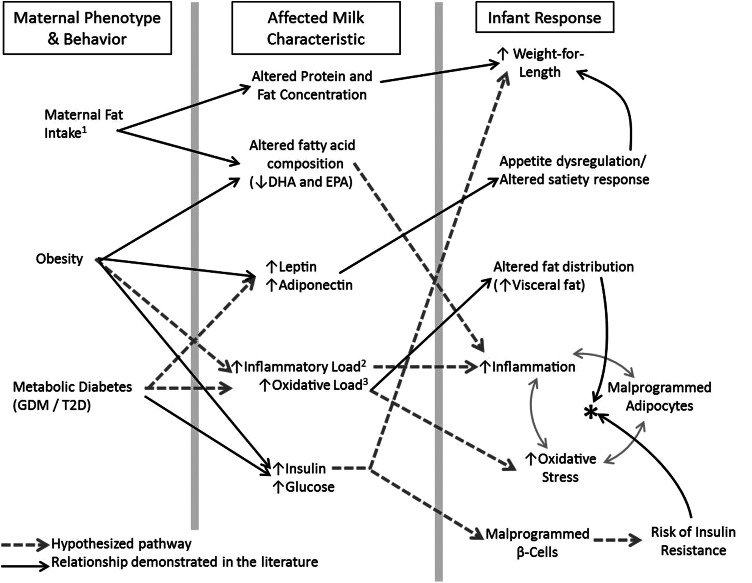
Childhood obesity rates have reached epidemic proportions. Excessive weight gain in infancy is associated with persistence of elevated weight status and later obesity. In this review, we make the case that weight gain in the first 6 mo is especially predictive of later obesity risk due to the metabolic programming that can occur early postpartum. The current state of knowledge regarding the biological determinants of excess infant weight gain is reviewed, with particular focus on infant feeding choice. Potential mechanisms by which different feeding approaches may program the metabolic profile of the infant, causing the link between early weight gain and later obesity are proposed. These mechanisms are likely highly complex and involve synergistic interactions between endocrine effects and factors that alter the inflammatory and oxidative stress status of the infant. Gaps in current knowledge are highlighted. These include a lack of data describing 1) what type of infant body fat distribution may impart risk and 2) how maternal metabolic dysfunction (obesity and/or diabetes) may affect milk composition and exert downstream effects on infant metabolism. Improved understanding and management of these early postnatal determinants of childhood obesity may have great impact on reducing its prevalence.
Conflict of interest statement
Author disclosures: B. E. Young, S. L. Johnson, and N. F. Krebs, no conflicts of interest.
Figures

References
-
- Flegal KM, Carroll MD, Kit BK, Ogden CL. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999–2010. JAMA. 2012;307:491–7 - PubMed
-
- Monteiro PO, Victora CG. Rapid growth in infancy and childhood and obesity in later life–a systematic review. Obes Rev. 2005;6:143–54 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
