

Progression of cartilage degradation, bone resorption and pain in rat temporomandibular joint osteoarthritis induced by injection of iodoacetate
- PMID: 22984604
- PMCID: PMC3439407
- DOI: 10.1371/journal.pone.0045036
Progression of cartilage degradation, bone resorption and pain in rat temporomandibular joint osteoarthritis induced by injection of iodoacetate
Abstract
Background: Osteoarthritis (OA) is an important subtype of temporomandibular disorders. A simple and reproducible animal model that mimics the histopathologic changes, both in the cartilage and subchondral bone, and clinical symptoms of temporomandibular joint osteoarthritis (TMJOA) would help in our understanding of its process and underlying mechanism.
Objective: To explore whether injection of monosodium iodoacetate (MIA) into the upper compartment of rat TMJ could induce OA-like lesions.
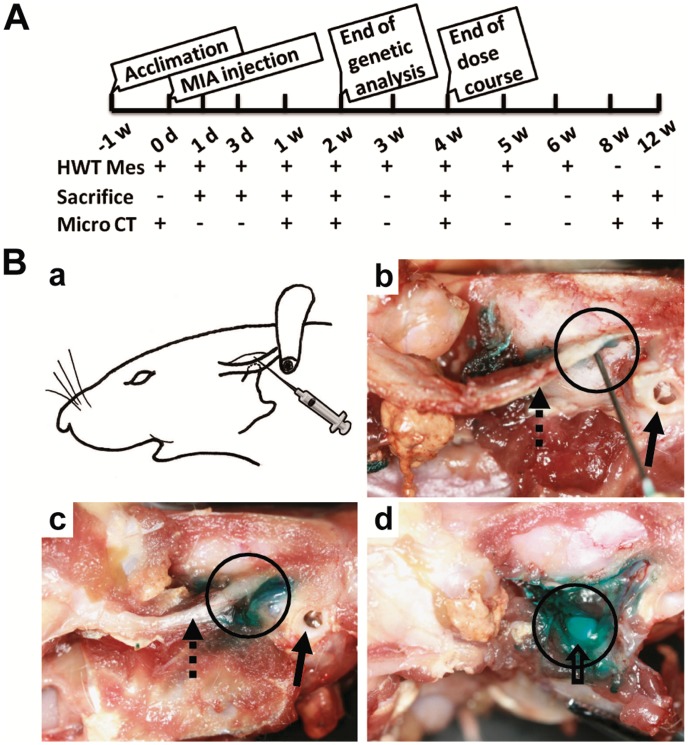
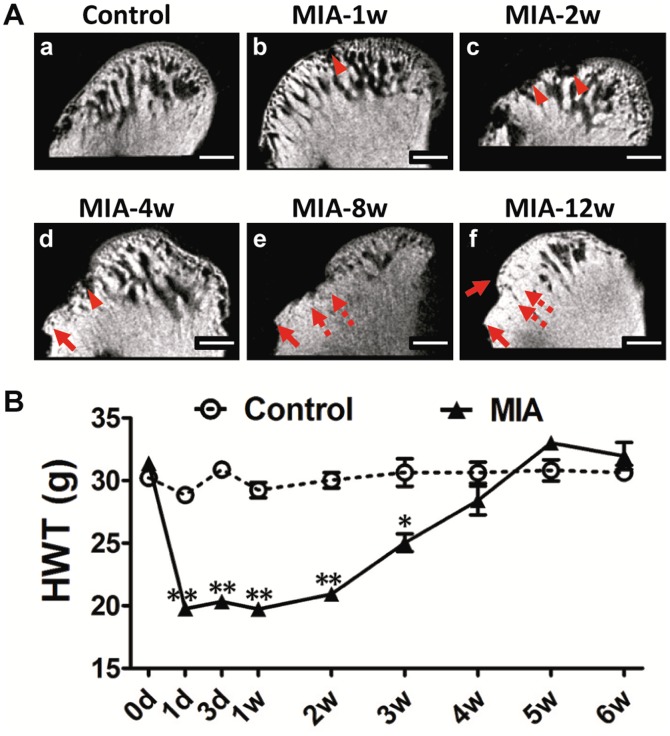
Methods: Female rats were injected with varied doses of MIA into the upper compartment and observed for up to 12 weeks. Histologic, radiographic, behavioral, and molecular changes in the TMJ were evaluated by light and electron microscopy, MicroCT scanning, head withdrawal threshold test, real-time PCR, immunohistochemistry, and TUNEL assay.
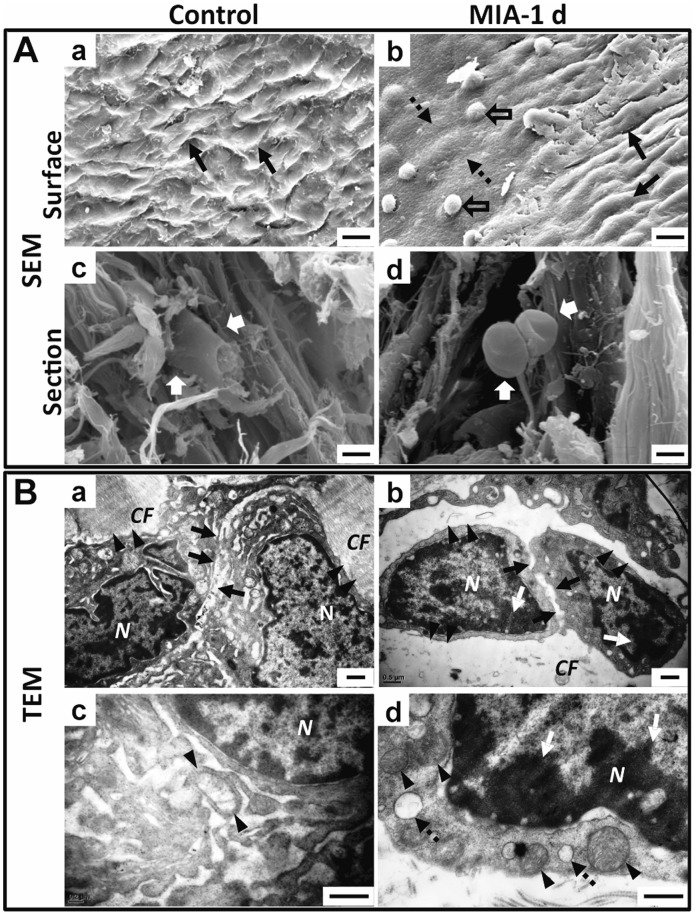
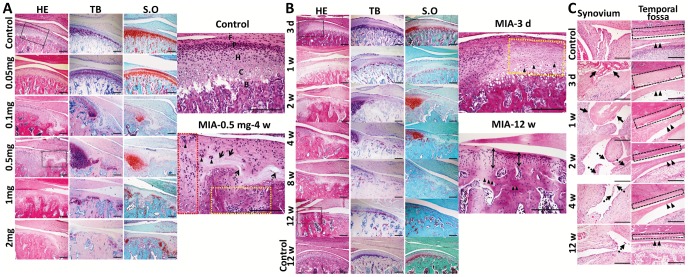
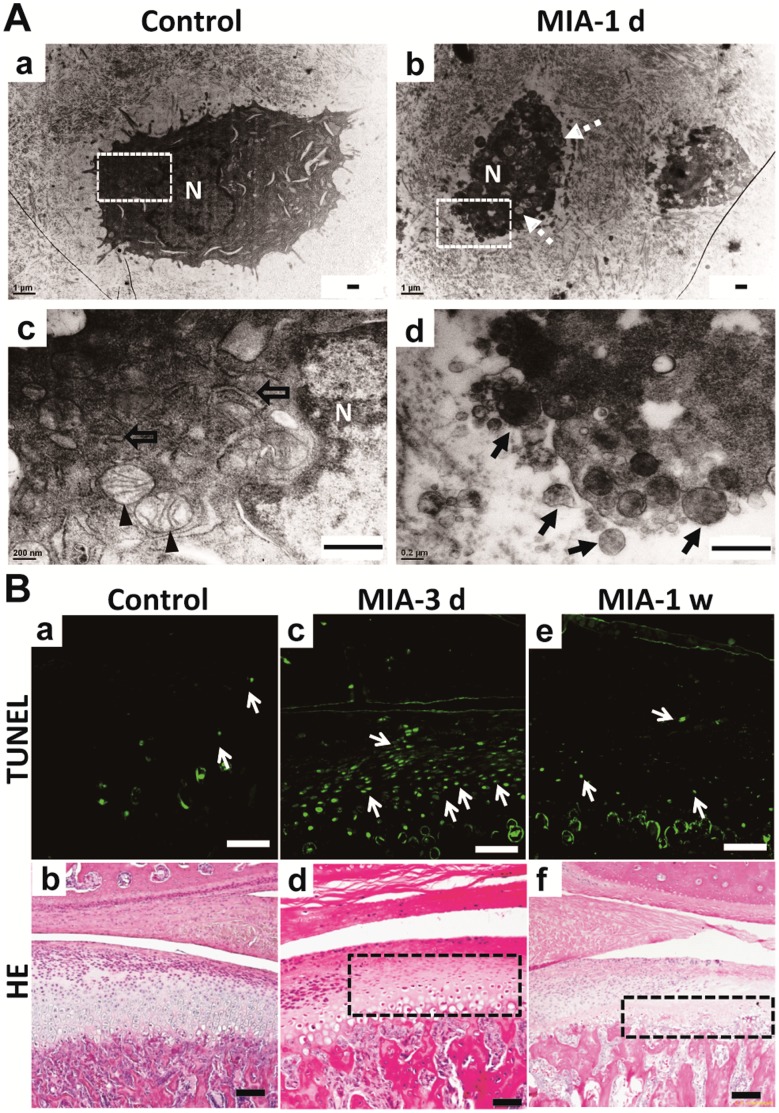
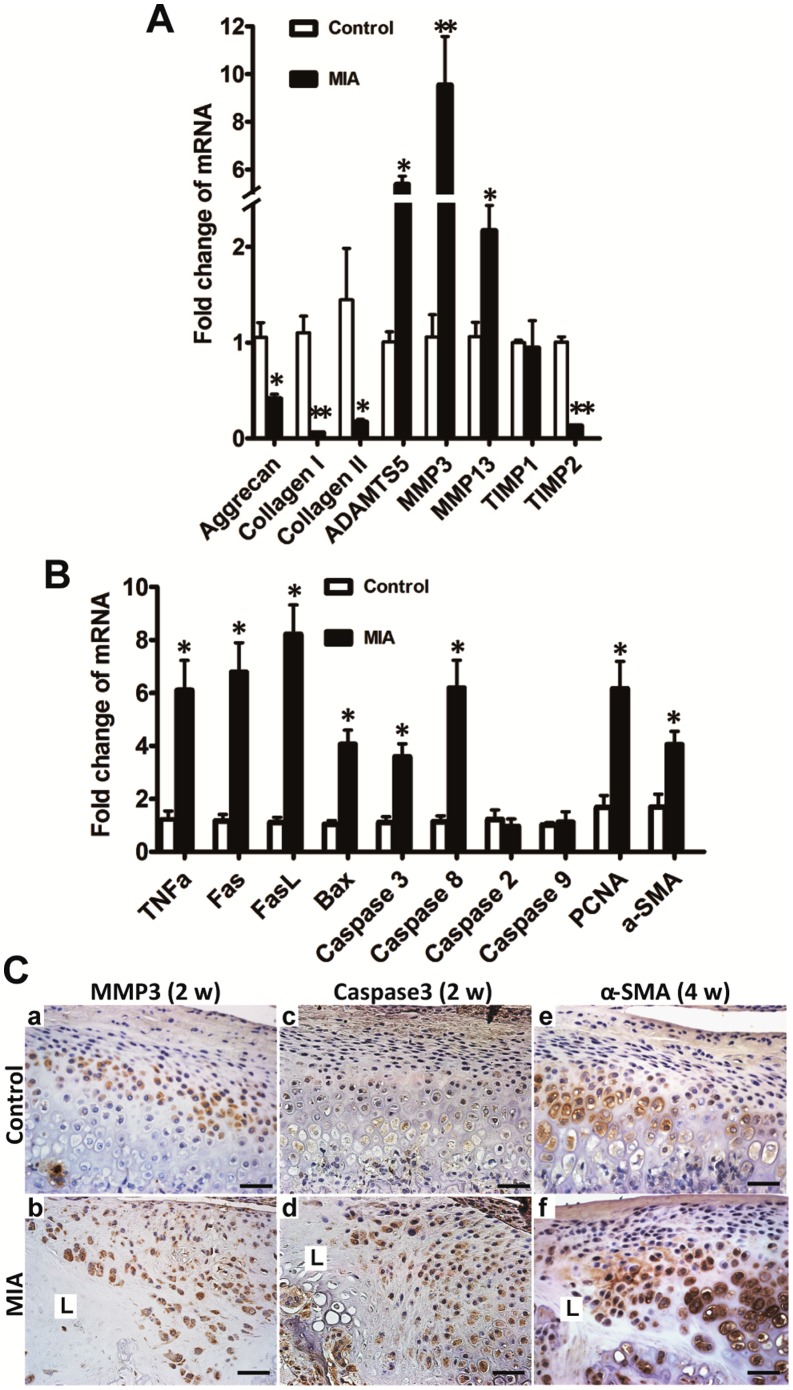
Results: The intermediate zone of the disc loosened by 1 day post-MIA injection and thinned thereafter. Injection of an MIA dose of 0.5 mg or higher induced typical OA-like lesions in the TMJ within 4 weeks. Condylar destruction presented in a time-dependent manner, including chondrocyte apoptosis in the early stages, subsequent cartilage matrix disorganization and subchondral bone erosion, fibrosis, subchondral bone sclerosis, and osteophyte formation in the late stages. Nociceptive responses increased in the early stages, corresponding to severe synovitis. Furthermore, chondrocyte apoptosis and an imbalance between anabolism and catabolism of cartilage and subchondral bone might account for the condylar destruction.
Conclusions: Multi-level data demonstrated a reliable and convenient rat model of TMJOA could be induced by MIA injection into the upper compartment. The model might facilitate TMJOA related researches.
Conflict of interest statement
Figures
References
-
- Dworkin SF, LeResche L (1992) Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord 6: 301–355. - PubMed
-
- Zarb GA, Carlsson GE (1999) Temporomandibular disorders: osteoarthritis. J Orofac Pain 13: 295–306. - PubMed
-
- Israel HA, Diamond B, Saed-Nejad F, Ratcliffe A (1998) Osteoarthritis and synovitis as major pathoses of the temporomandibular joint: comparison of clinical diagnosis with arthroscopic morphology. J Oral Maxillofac Surg 56: 1023–1027; discussion 1028. - PubMed
-
- Stegenga B, de Bont LG, Boering G (1989) Osteoarthrosis as the cause of craniomandibular pain and dysfunction: a unifying concept. J Oral Maxillofac Surg 47: 249–256. - PubMed
-
- Karsdal MA, Leeming DJ, Dam EB, Henriksen K, Alexandersen P, et al. (2008) Should subchondral bone turnover be targeted when treating osteoarthritis? Osteoarthritis Cartilage 16: 638–646. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
