A comparison of preplan MRI and preplan CT-based prostate volume with intraoperative ultrasound-based prostate volume in real-time permanent brachytherapy
- PMID: 22984671
- PMCID: PMC3429903
- DOI: 10.3857/roj.2011.29.3.199
A comparison of preplan MRI and preplan CT-based prostate volume with intraoperative ultrasound-based prostate volume in real-time permanent brachytherapy
Abstract
Purpose: The present study compared the difference between intraoperative transrectal ultrasound (iTRUS)-based prostate volume and preplan computed tomography (CT), preplan magnetic resonance imaging (MRI)-based prostate volume to estimate the number of seeds needed for appropriate dose coverage in permanent brachytherapy for prostate cancer.
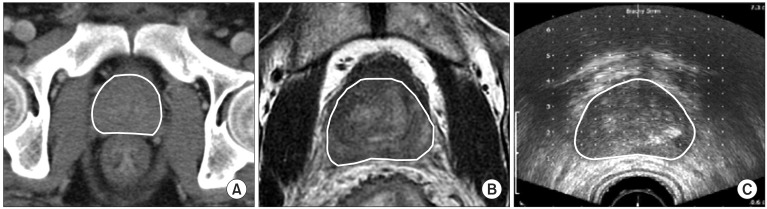
Materials and methods: Between March 2007 and March 2011, among 112 patients who underwent permanent brachytherapy with (125)I, 60 image scans of 56 patients who underwent preplan CT (pCT) or preplan MRI (pMRI) within 2 months before brachytherapy were retrospectively reviewed. Twenty-four cases among 30 cases with pCT and 26 cases among 30 cases with pMRI received neoadjuvant hormone therapy (NHT). In 34 cases, NHT started after acquisition of preplan image. The median duration of NHT after preplan image acquisition was 17 and 21 days for cases with pCT and pMRI, respectively. The prostate volume calculated by different modalities was compared. And retrospective planning with iTRUS image was performed to estimate the number of (125)I seed required to obtain recommended dose distribution according to prostate volume.
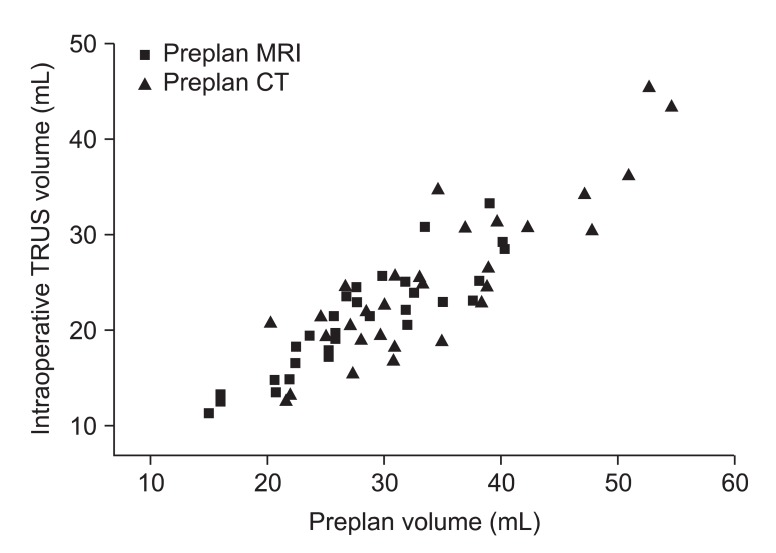
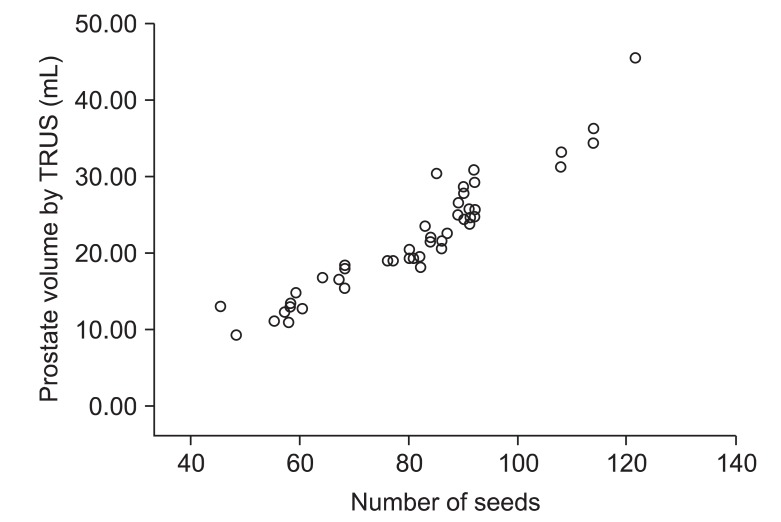
Results: The mean difference in prostate volume was 9.05 mL between the pCT and iTRUS and 6.84 mL between the pMRI and iTRUS. The prostate volume was roughly overestimated by 1.36 times with pCT and by 1.33 times with pMRI. For 34 cases which received NHT after image acquisition, the prostate volume was roughly overestimated by 1.45 times with pCT and by 1.37 times with pMRI. A statistically significant difference was found between preplan image-based volume and iTRUS-based volume (p < 0.001). The median number of wasted seeds is approximately 13, when the pCT or pMRI volume was accepted without modification to assess the required number of seeds for brachytherapy.
Conclusion: pCT-based volume and pMRI-based volume tended to overestimate prostate volume in comparison to iTRUS-based volume. To reduce wasted seeds and cost of the brachytherapy, we should take the volume discrepancy into account when we estimate the number of (125)I seeds for permanent brachytherapy.
Keywords: Brachytherapy; Prostate cancer; Prostate volume.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Polo A, Salembier C, Venselaar J, Hoskin P PROBATE group of the GEC ESTRO. Review of intraoperative imaging and planning techniques in permanent seed prostate brachytherapy. Radiother Oncol. 2010;94:12–23. - PubMed
-
- Ishiyama H, Nakamura R, Satoh T, et al. Differences between intraoperative ultrasound-based dosimetry and postoperative computed tomography-based dosimetry for permanent interstitial prostate brachytherapy. Brachytherapy. 2010;9:219–223. - PubMed
-
- Hinnen KA, Battermann JJ, van Roermund JG, et al. Long-term biochemical and survival outcome of 921 patients treated with I-125 permanent prostate brachytherapy. Int J Radiat Oncol Biol Phys. 2010;76:1433–1438. - PubMed
-
- Zelefsky MJ, Hollister T, Raben A, Matthews S, Wallner KE. Five-year biochemical outcome and toxicity with transperineal CT-planned permanent I-125 prostate implantation for patients with localized prostate cancer. Int J Radiat Oncol Biol Phys. 2000;47:1261–1266. - PubMed
-
- Stock RG, Cesaretti JA, Stone NN. Disease-specific survival following the brachytherapy management of prostate cancer. Int J Radiat Oncol Biol Phys. 2006;64:810–816. - PubMed
LinkOut - more resources
Full Text Sources