Helical tomotherapy for spine oligometastases from gastrointestinal malignancies
- PMID: 22984674
- PMCID: PMC3429906
- DOI: 10.3857/roj.2011.29.4.219
Helical tomotherapy for spine oligometastases from gastrointestinal malignancies
Abstract
Purpose: This study evaluated the treatment effectiveness and proper radiation dose of helical tomotherapy (HT) in spine oligometastases from gastrointestinal cancers.
Materials and methods: From 2006 to 2010, 20 gastrointestinal cancer patients were treated with HT for spine oligometastases (31 spine lesions). The gross tumor volume (GTV) was the tumor evident from magnetic resonance imaging images fused with simulation computed tomography images. Clinical target volume (CTV) encompassed involved vertebral bodies or dorsal elements. We assumed that the planning target volume was equal to the CTV. We assessed local control rate after HT for 31 spine metastases. Pain response was scored by using a numeric pain intensity scale (NPIS, from 0 to 10).
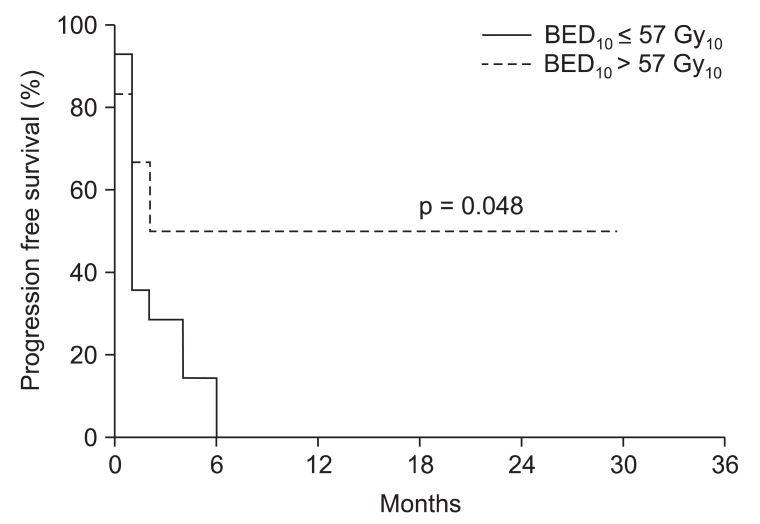
Results: Spine metastatic lesions were treated with median dose of 40 Gy (range, 24 to 51 Gy) and median 5 Gy per fraction (range, 2.5 to 8 Gy) to GTV with median 8 fractions (range, 3 to 20 fraction). Median biologically equivalent dose (BED, α/β = 10 Gy) was 52 Gy(10) (range, 37.5 to 76.8 Gy(10)) to GTV. Six month local control rate for spine metastasis was 90.3%. Overall infield failure rate was 15% and outfield failure rate was 75%. Most patients showed pain relief after HT (93.8%). Median local recurrence free survival was 3 months. BED over 57 Gy(10) and oligometastases were identified as prognostic factors associated with improved local progression free survival (p = 0.012, p = 0.041).
Conclusion: HT was capable of delivering higher BED to metastatic lesions in close proximity of the spinal cord. Spine metastases from gastrointestinal tumors were sensitive to high dose radiation, and BED (α/β = 10 Gy) higher than 57 Gy(10) could improve local control.
Keywords: Helical tomotherapy; Spine metastasis.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures




References
-
- Ratliff JK, Cooper PR. Metastatic spine tumors. South Med J. 2004;97:246–253. - PubMed
-
- Foro Arnalot P, Fontanals AV, Galceran JC, et al. Randomized clinical trial with two palliative radiotherapy regimens in painful bone metastases: 30 Gy in 10 fractions compared with 8 Gy in single fraction. Radiother Oncol. 2008;89:150–155. - PubMed
-
- Kaizu T, Karasawa K, Tanaka Y, et al. Radiotherapy for osseous metastases from hepatocellular carcinoma: a retrospective study of 57 patients. Am J Gastroenterol. 1998;93:2167–2171. - PubMed
-
- Sahgal A, Bilsky M, Chang EL, et al. Stereotactic body radiotherapy for spinal metastases: current status, with a focus on its application in the postoperative patient. J Neurosurg Spine. 2011;14:151–166. - PubMed
-
- Thariat J, Marcy PY, Lagrange JL. Trends in radiation therapy for the treatment of metastatic and oligometastatic disease in 2010. Bull Cancer. 2010;97:1467–1476. - PubMed
LinkOut - more resources
Full Text Sources